Chapter: Medical Surgical Nursing: Assessment of Musculoskeletal Function
Structure and Function of the Skeletal Muscle System
STRUCTURE AND FUNCTION OF THE SKELETAL MUSCLE
SYSTEM
Muscles are attached by tendons (cords of fibrous connective
tis-sue) or aponeuroses (broad, flat sheets of connective tissue) to bones,
connective tissue, other muscles, soft tissue, or skin. The muscles of the body
are composed of parallel groups of muscle cells (fasciculi) encased in fibrous
tissue called fascia or epimy-sium. The more fasciculi
contained in a muscle, the more precisethe movements. Muscles vary in shape and
size according to the activities for which they are responsible. Skeletal
(striated) muscles are involved in body movement, posture, and heat-production
functions. Muscles contract to bring the two points of attach-ment closer
together, resulting in movement.
Skeletal Muscle Contraction
Each muscle cell (also
referred to as a muscle fiber) contains myo-fibrils, which in turn are composed
of a series of sarcomeres, the actual contractile units of skeletal muscle.
Sarcomeres contain thick myosin and thin actin filaments. Muscle fibers
contract in response to electrical stimulation de-livered by an effector nerve
cell at the motor end plate. When stim-ulated, the muscle cell depolarizes and
generates an action potential in a manner similar to that described for nerve
cells. These action potentials propagate along the muscle cell membrane and
lead to the release of calcium ions that are stored in specialized organelles
called the sarcoplasmic reticulum. When there is a local increase in calcium
ion concentration, the myosin and actin filaments slide across one another.
Shortly after the muscle cell membrane is de-polarized, it recovers its resting
membrane voltage. Calcium is rapidly removed from the sarcomeres by active
reaccumulation in the sarcoplasmic reticulum. When calcium concentration in the
sarcomere decreases, the myosin and actin filaments cease to inter-act, and the
sarcomere returns to its original resting length (relax-ation). Actin and
myosin do not interact in the absence of calcium.
Energy is consumed
during muscle contraction and relax-ation. The primary source of energy for the
muscle cells is adeno-sine triphosphate (ATP), which is generated through
cellular oxidative metabolism. At low levels of activity (ie, sedentary
ac-tivity), the skeletal muscle synthesizes ATP from the oxidation of glucose
to water and carbon dioxide. During periods of strenu-ous activity, when
sufficient oxygen may not be available, glucose is metabolized primarily to
lactic acid, an inefficient process com-pared with that of oxidative pathways.
Stored muscle glycogen is used to supply glucose during periods of activity.
Muscle fatigue is thought to be caused by depletion of glycogen and
accumula-tion of lactic acid. As a result, the cycle of muscle contraction and
relaxation cannot continue.
During muscle contraction, the energy released from ATP
is not completely used. The excess energy is dissipated in the form of heat.
During isometric contraction, almost all of the energy is released in the form
of heat; during isotonic contraction, some of the energy is expended in
mechanical work. In some situations, such as shivering because of cold, the
need to generate heat is the primary stimulus for muscle contraction.
Types of Muscle Contractions
The contraction of
muscle fibers can result in either isotonic or iso-metric contraction of the
muscle. In isometric contraction,
the length of the muscles remains constant but the force generated by the
muscles is increased; an example of this is when one pushes against an
immovable wall. Isotonic contraction,
on the other hand, is characterized by shortening of the muscle with no
increase in tension within the muscle; an example of this is flexion of the
forearm. In normal activities, many muscle movements are a com-bination of
isometric and isotonic contraction. For example, during walking, isotonic
contraction results in shortening of the leg, and isometric contraction causes
the stiff leg to push against the floor.
The speed of the muscle
contraction is variable. Myoglobulin is a hemoglobin-like protein pigment
present in striated muscle cells that transports oxygen. Muscles containing
large quantities of myoglobulin (red muscles) have been observed to contract
slowly and powerfully (eg, respiratory and postural muscles). Muscles
containing little myoglobulin (white muscles) contract quickly (eg, extraocular
eye muscles). Most muscles contain both red and white muscle fibers.
Muscle Tone
Relaxed muscles
demonstrate a state of readiness to respond to contraction stimuli. This state
of readiness, known as muscle tone
(tonus), is produced by the maintenance of some of the muscle fibers in a contracted state. Muscle
spindles, which are sense organs in the muscles, monitor muscle tone. Muscle
tone is minimal during sleep and is increased when the person is anxious. A
muscle that is limp and without tone is described as flaccid; a muscle with greater-than-normal tone is described as spastic. In conditions characterized by
lower motor neuron destruction (eg, polio), denervated muscle becomes atonic (soft and flabby) and atrophies.
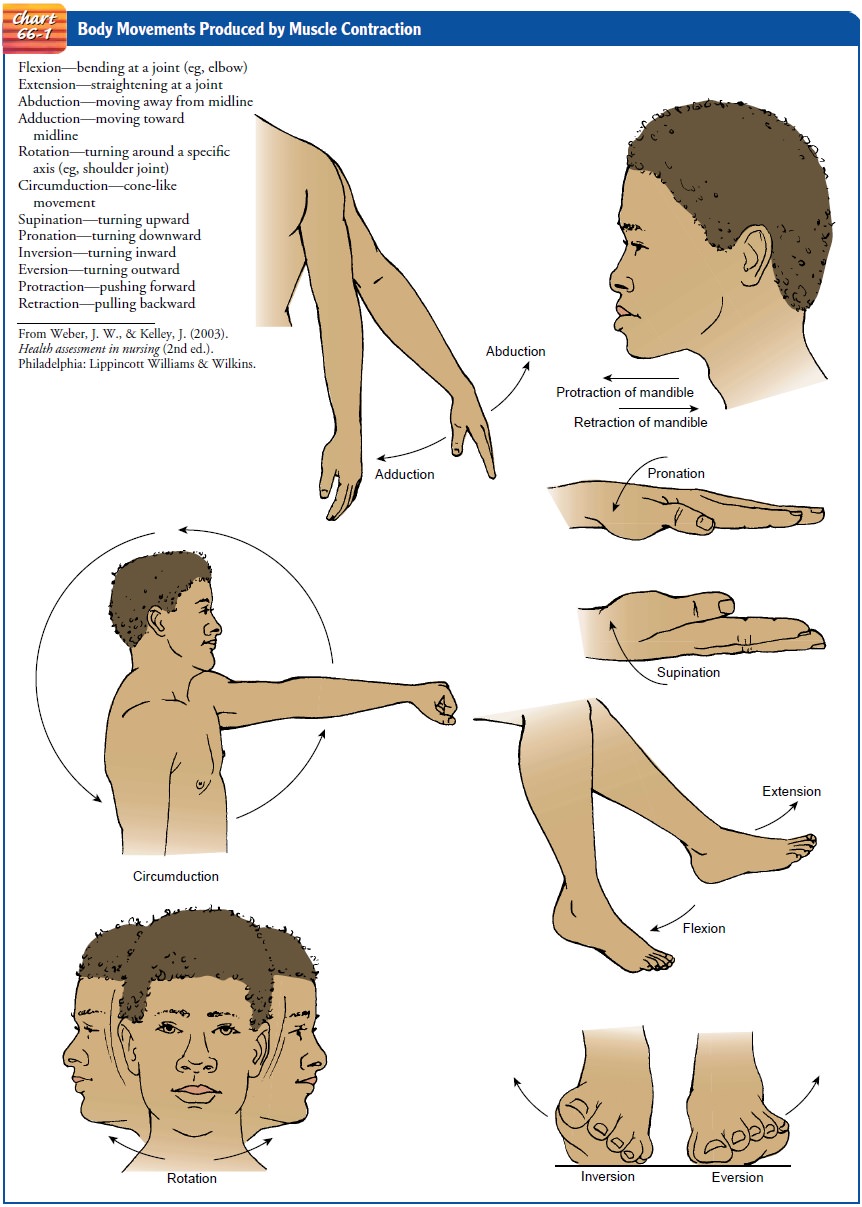
Muscle Actions
Muscles accomplish
movement by contraction. Through the co-ordination of muscle groups, the body
is able to perform a wide variety of movements (Chart 66-1). The prime mover is
the mus-cle that causes a particular motion. The muscles assisting the prime
mover are known as synergists. The muscles causing move-ment opposite to that
of the prime mover are known as antago-nists. An antagonist must relax to allow
the prime mover to contract, producing motion. For example, when contraction of
the biceps causes flexion of the elbow joint, the biceps is the prime mover,
and the triceps is the antagonist. A person with muscle paralysis, which is a loss of movement possibly from nerve dam-age,
may be able to retrain functioning muscles within the syner-gistic group to
produce the needed movement. Muscles of the synergistic group then become the
prime mover.
Exercise, Disuse, and Repair
Muscles need to be
exercised to maintain function and strength. When a muscle repeatedly develops
maximum or close to maxi-mum tension over a long time, as in regular exercise
with weights, the cross-sectional area of the muscle increases. This
enlargement, known as hypertrophy,
results from an increase in the size of in-dividual muscle fibers without an
increase in the number of mus-cle fibers. Hypertrophy persists only if the
exercise is continued. The opposite phenomenon occurs with disuse of muscle
over a long period of time. Age and disuse cause loss of muscular func-tion as
fibrotic tissue replaces the contractile muscle tissue. The decrease in the
size of a muscle is called atrophy.
Bed rest and im-mobility cause loss of muscle mass and strength. When
immo-bility is the result of a treatment mode (eg, casting, traction), the
patient can decrease the effects of immobility by isometric exer-cise of the
muscles of the immobilized part. Quadriceps setting exercises (tightening the
muscles of the thigh) and gluteal setting exercises (tightening of the muscles
of the buttocks) help main-tain the larger muscle groups that are important in
ambulation. Active and weight-resistance exercises of uninjured parts of the
body maintain muscle strength. When muscles are injured, they need rest and
immobilization until tissue repair occurs. The healed muscle then needs
progressive exercise to resume its pre-injury strength and functional ability.
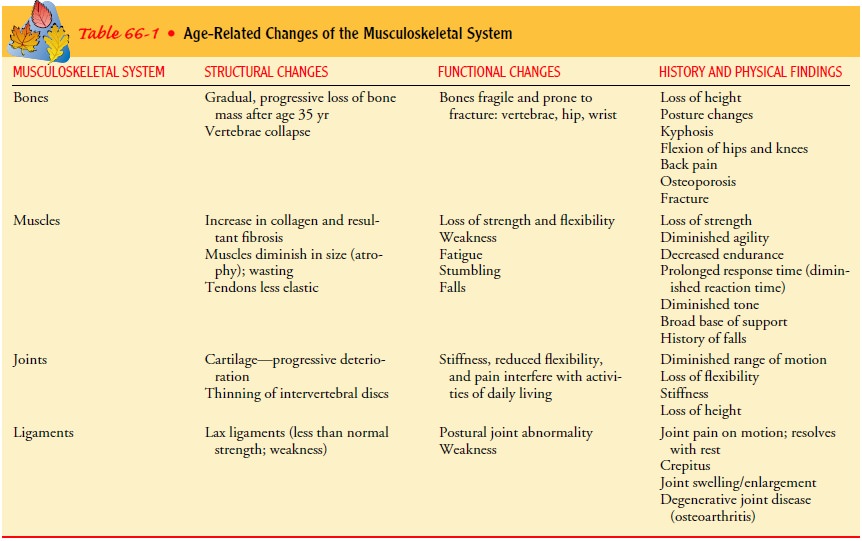
Gerontologic Considerations
Multiple changes in the
musculoskeletal system occur with aging (Table 66-1). Bone mass peaks at about
35 years of age, after which there is a universal gradual loss of bone. There
is a loss of height due to osteoporosis (abnormal excessive bone loss),
kypho-sis, thinned intervertebral disks, and flexion of the knees and hips.
Numerous metabolic changes, including menopausal withdrawal of estrogen and
decreased activity, contribute to osteoporosis. Women lose more bone mass than
men do. Additionally, bones change in shape and have reduced strength.
Fractures are common. In the elderly, collagen structures are less able to
absorb en-ergy. Ligaments become weak. The articular cartilage degenerates in
weight-bearing areas and heals less readily. This contributes to the
development of osteoarthritis. Joints enlarge and range of motion decreases.
Muscle mass and strength are also diminished. There is an actual loss in the
size and number of muscle fibers due to myofibril atrophy with fibrous tissue
replacement. Increased in-activity, diminished neuron stimulation, and nutritional
defi-ciencies contribute to loss of muscle strength. In addition, remote
musculoskeletal problems for which the patient has compensated may become new
problems with age-related changes. For example, people who have had polio and
who have been able to function normally by using synergistic muscle groups may
discover increas-ing incapacity because of a reduced compensatory ability. Many
of the effects of aging, however, can be slowed if the body is kept healthy and
active through positive lifestyle behaviors.
Related Topics