Chapter: Clinical Anesthesiology: Clinical Pharmacology: Anticholinergic Drugs
Specific Anticholinergic Drugs
Specific Anticholinergic Drugs
ATROPINE
Physical Structure
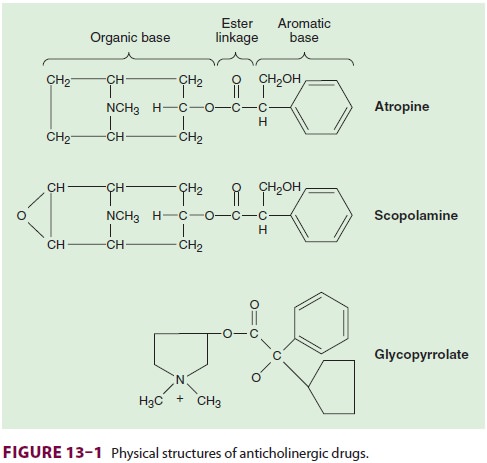
Atropine is a tertiary amine. The naturally
occurring levorotatory form is active, but the commercial mix-ture is racemic
(Figure 13–1).
Dosage & Packaging
As a premedication, atropine is
administered intra-venously or intramuscularly in a range of 0.01–0.02 mg/kg,
up to the usual adult dose of 0.4–0.6 mg. Larger intravenous doses up to 2 mg
may be required to completely block the cardiac vagal nerves in treat-ing
severe bradycardia. Atropine sulfate is available in a multitude of
concentrations.
Clinical Considerations
Atropine has particularly potent eff
ects on the heart and bronchial smooth muscle and is themost efficacious
anticholinergic for treating brady-arrhythmias. Patients with coronary artery
disease may not tolerate the increased myocardial oxygen demand and decreased
oxygen supply associated with the tachycardia caused by atropine. A derivative
of atropine, ipratropium bromide, is available in a metered-dose inhaler for
the treatment of broncho-spasm. Its quaternary ammonium structure significantly
limits systemic absorption. Ipratropium solution (0.5 mg in 2.5 mL) seems to be
particularly effective in the treatment of acute chronic obstructive pulmonary
disease when combined with a β-agonist drug (eg, albuterol). The
central nervoussystem effects of atropine are minimal after
the usual doses, even though this tertiary amine can rapidly cross the
blood–brain barrier. Atropine has been associated with mild postoperative
memory deficits, and toxic doses are usually associated with excit-atory
reactions. An intramuscular dose of 0.01– 0.02 mg/kg reliably provides an
antisialagogue effect. Atropine should be used cautiously in patients with
narrow-angle glaucoma, prostatic hypertrophy, or bladder-neck obstruction.
SCOPOLAMINE
Physical Structure
Scopolamine, a tertiary amine, differs
from atropine by the addition of an epoxide to the heterocyclic ring.
Dosage & Packaging
The premedication dose of scopolamine is
the same as that of atropine, and it is usually given intramus-cularly.
Scopolamine hydrobromide is available as solutions containing 0.3, 0.4, and 1
mg/mL.
Clinical Considerations
Scopolamine is a more potent
antisialagogue than atropine and causes greater central nervous system effects.
Clinical dosages usually result in drowsiness and amnesia, although
restlessness, diz-ziness, and delirium are possible. The sedative effects may
be desirable for premedication but can interfere with awakening following short
procedures. Scopol-amine has the added virtue of preventing motion sickness.
The lipid solubility allows transdermal absorption, and transdermal scopolamine
has been used to prevent postoperative nausea and vomiting. Because of its
pronounced ocular effects, scopol-amine is best avoided in patients with
closed-angle glaucoma.
GLYCOPYRROLATE
Physical Structure
Glycopyrrolate is a synthetic product
that differs from atropine in being a quaternary amine and having both
cyclopentane and a pyridine moieties in the compound
Dosage & Packaging
The usual dose of glycopyrrolate is
one-half that of atropine. For instance, the premedication dose is 0.005–0.01
mg/kg up to 0.2–0.3 mg in adults. Gly-copyrrolate for injection is packaged as
a solution of 0.2 mg/mL.
Clinical Considerations
Because of its quaternary structure,
glycopyr-rolate cannot cross the blood–brain barrierand is almost devoid of
central nervous system and ophthalmic activity. Potent inhibition of salivary
gland and respiratory tract secretions is the primary rationale for using
glycopyrrolate as a premedication. Heart rate usually increases after
intravenous—but not intramuscular—administration. Glycopyrrolate has a longer
duration of action than atropine (2–4 h vs 30 min after intravenous
administration)
Related Topics