Chapter: Modern Pharmacology with Clinical Applications: Adrenomimetic Drugs
Pharmacological Actions of Dopamine
PHARMACOLOGICAL
ACTIONS OF DOPAMINE
Dopamine is a naturally
occurring catecholamine; it is the immediate biochemical precursor of the
norepi-nephrine found in adrenergic neurons and the adrenal medulla. It is also
a neurotransmitter in the CNS, where it is released from dopaminergic neurons
to act on spe-cific dopamine receptors .
Dopamine is a unique
adrenomimetic drug in that it exerts its cardiovascular actions by (1)
releasing norepi-nephrine from adrenergic neurons, (2) interacting with α-and β1-adrenoceptors, and (3)
interacting with spe-cific dopamine receptors.
The cardiovascular response
to dopamine in hu-mans depends on the concentration infused. Low rates of
dopamine infusion can produce vasodilation in the renal, mesenteric, coronary,
and intercerebral vascular beds with little effect on other blood vessels or on
the heart. The vasodilation produced by dopamine is not antagonized by the β-adrenoceptor blocking agent
pro-pranolol but is antagonized by haloperidol and other dopamine
receptor–blocking agents.
Dopamine can exert pronounced
cardiovascular and renal effects through the activation of both D1-
and D2-receptor subtypes. Stimulation of the D1-receptor,
which is present on blood vessels and certain other pe-ripheral sites, will
result in vasodilation, natriuresis, and diuresis. D2-receptors are
found on ganglia, on sympa-thetic nerve terminals, on the adrenal cortex, and
within the cardiovascular centers of the CNS; their activation produces
hypotension, bradycardia, and regional va-sodilation (e.g., renal
vasodilation). The kidney appears to be a particularly rich source for endogenous
dopamine in the periphery.
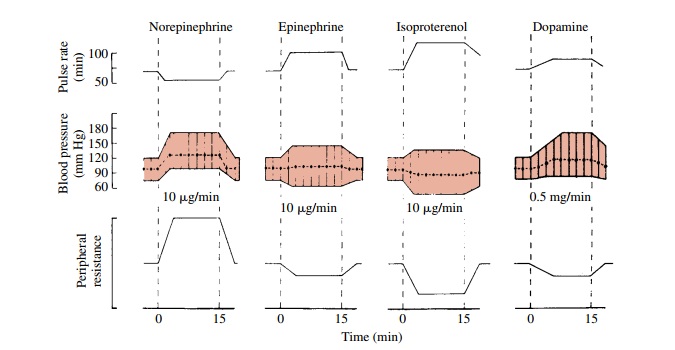
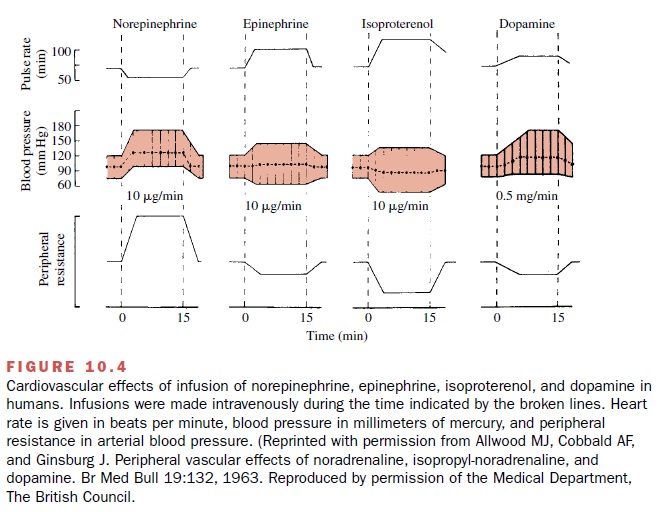
The infusion of moderately
higher concentrations of dopamine increases the rate and contractile force of
the heart and augments the cardiac output. This action is mediated by β 1-adrenoceptors and
norepinephrine re-lease and is antagonized by propranolol. In contrast to
isoproterenol, which has a marked effect on both the rate and the contractile
force of the heart, dopamine has a greater effect on the force than on cardiac
rate. The advantage of this greater inotropic than chronotropic effect of
dopamine is that it produces a smaller increase in oxygen demand by the heart
than does isoproterenol. Systolic blood pressure is increased by dopamine,
whereas diastolic pressure is usually not changed signif-icantly. Total
peripheral resistance is decreased because of the vasodilator effect of
dopamine (Fig. 10.4).
At still higher
concentrations, dopamine causes α-adrenoceptor-mediated vasoconstriction in most
vas-cular beds and stimulates the heart. Total peripheral re-sistance may be increased.
If the concentration of dopamine reaching the tissue is high enough,
vasocon-striction of the renal and mesenteric beds also occurs. The
vasoconstrictive action of dopamine is antagonized by α-adrenoceptor blocking agents
such as phentol-amine.
Related Topics