Chapter: Essentials of Psychiatry: Behavior and Adaptive Functioning
Personality Style
Behavior and Adaptive Functioning
To function adaptively means to behave in such a way that one’s attitudes and actions are well matched to the demands and con-straints of the external environment and that one’s sense of inter-nal discomfort or distress is minimized. Therefore, by definition, the ability to adapt depends both on the individual’s behavioral repertoire and on the external environment. A person’s capacity for adaptive functioning is so crucial that it has been studied in situations ranging from adaptation to long-term missions in outer space (Eksuzian, 1999) to the self-management of life-threaten-ing illnesses such as chronic heart failure (Buetow et al., 2001).
Personality Style
An individual’s personality style has a great
influence on his or her behavior and adaptive functioning. Personality is
shaped from a blend of inborn temperament, genetic strengths and
vulnerabilities, and the impact of positive and negative life experiences.
Psychiatry is moving toward an improved understanding of human behavior that
focuses on the ways that these factors interact with one another.
There is evidence of striking variation among
neonates in their capacity to tolerate frustration, which reflects their inborn
temperaments (Thomas et al., 1963).
Such individual differences in temperament form the biological substrate that
interacts with early development. Temperament affects the degree to which
different infants are susceptible to distress as well as their variations in
attachment style (Rothbart and Ahadi, 1994).
Genetic factors of various types also play a role
in develop-ment, particularly when they interact with environmental factors. In
general, genetic factors account for between 30 and 60% of the variance in
adult personality traits (Carey and DiLalla, 1994).
Life experiences also have an impact on an
individual and affect her or his behavior for better or worse. Considering
whether particular experiences are the result of fate in contrast to whether
they are partially brought about by the person’s own actions can be important
in thinking about their impact and meaning.
While psychiatrists have long suspected links
between early life experiences, especially traumatic ones, and adult
psychopathology, these connections are just now being clearly, empirically
demonstrated. For example, in one recent study, childhood verbal abuse
conferred an increased likelihood of borderline, narcissistic, paranoid,
schizoid and schizotypal per-sonality disorder during adolescence which was
independent of other facts like temperament, physical and sexual abuse, use of
corporal punishment, parental psychopathology and cooccuring psychiatric
disorders (Johnson et al., 2001).
Further, as the rela-tionships between genetic propensities expressed as
temperament or personality factors and environmental influences have been
explicated, some fascinating interactions have emerged. For ex-ample, one
recent study suggested that high levels of the person-ality trait of sensation
seeking, which appears to be genetically mediated, might result in a high
incidence of adverse life events that would in turn help to precipitate
depression (Farmer et al., 2001)
Further, exploration of patterns of disease and personality factors is
beginning to shape genetic investigations by serving as guides for genetic
linkage studies (Nigg and Goldsmith, 1998). For instance, in one study, twins
and siblings who were highly concordant and discordant for neuroticism, a
personality factor, were examined for evidence of anxiety and depression.
Tissue samples were collected to look for areas of genetic overlap and thus to
identify potential foci on chromosomes that warranted further exploration (Kirk
et al., 2000).
Personality styles have been described in a variety
of ways with use of different models of normal personality varia-tion. These
models are either categorical or dimensional in na-ture. In a categorical
model, a person is described as meeting or not meeting the criteria for various
diagnostic categories. In a dimensional model of personality, a person is
evaluated in terms of the blend of various traits or factors he or she
pos-sesses, measured on a continuum. In general, as a person moves toward the
extreme end of a given continuum in the dimensional model, she or he becomes
more likely to meet the criteria for a categorical diagnosis. Some dimensional
models set a threshold beyond which a given characteristic is likely to be a
problem or pathological.
The categorical model is a more common approach to
diag-nosis within clinical psychiatry and within medicine in general. It now
seems clear that useful information is gained from both categorical and
dimensional approaches to examining personal-ity. Thus, although personality
disorders as outlined in the Diag-nostic
and Statistical Manual of Mental Disorders, Fourth Edi-tion (DSM-IV-TR)
(American Psychiatric Association, 1994) are currently cast in categorical
terms, Oldham and Skodol (2000), among others, have suggested that elements of
both categorical and dimensional systems be included when revisions are made in
DSM-V. Others have proposed a prototype-matching approach to diagnosing
personality disorders in which models of various per-sonality styles are
constructed and psychiatrists make diagnosis by matching their patient to the
best available prototype (Westen and Shedler, 2000).
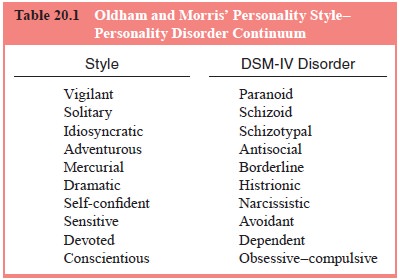
Oldham and Morris (1995) translated each of the
person-ality disorders of the DSM-IV-TR system into a less pathological
collection of categories that describe normal personality styles. In their
system, a cross between a categorical and a dimensional model,
conscientiousness is the positive personality trait that in excess becomes
obsessive–compulsive personality disorder. Table 20.1 summarizes the
personality style–personality disor-der continuum described by Oldham and Morris.
A continuum model such as this one acknowledges
that whereas too much of a good thing may constitute a disorder, everyone’s
personality consists of traits that can be adaptive or maladaptive. The
quantity rather than the quality of a given trait
is often what makes it a problem or adaptive.
Similarly, flexibility and variability are important determinants of a person’s
adaptive capacity.
Examples of dimensional models of personality
in-clude the five-factor model (Widiger et
al., 1994), Cloninger’s seven-factor model (Cloninger, 1987; Cloninger et al., 1993), and the biogenic spectrum
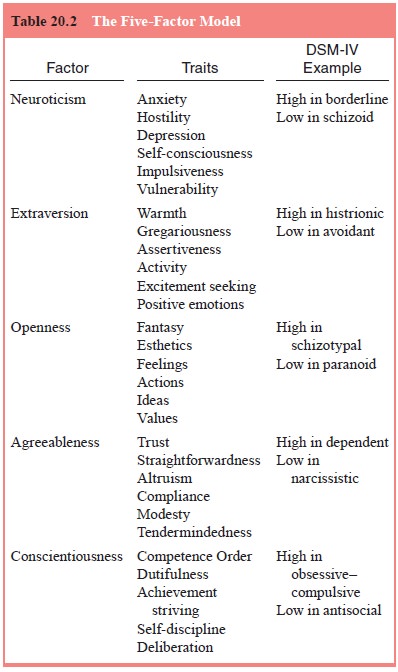
model of Siever and Davis (1991). The five-factor model of personality was
first suggested by McDougall (1932) and was elaborated and updated by Dig-man
(1990) and McCrae and Costa (1987) among others. In the five-factor model,
personality traits are described in terms of a taxonomy of five dimensions.
These include neu-roticism, extraversion, openness to experience, agreeableness
and conscientiousness. Table 20.2 summarizes the factors of the five-factor
model and their relationship to DSM-IV-TR categories.
A second dimensional model of personality is
Cloninger’s seven-factor model of temperament and character (Cloninger, 1987;
Cloninger et al., 1993) (Table 20.3).
In this model, a pa-tient’s behavior is evaluated on seven separate dimensions.
Four of the seven dimensions are related to temperament and have been shown to
be independently heritable, manifested early in life, and involved in early perceptual
memory and habit formation
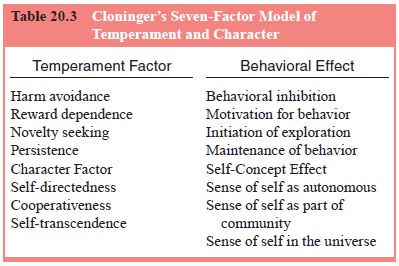
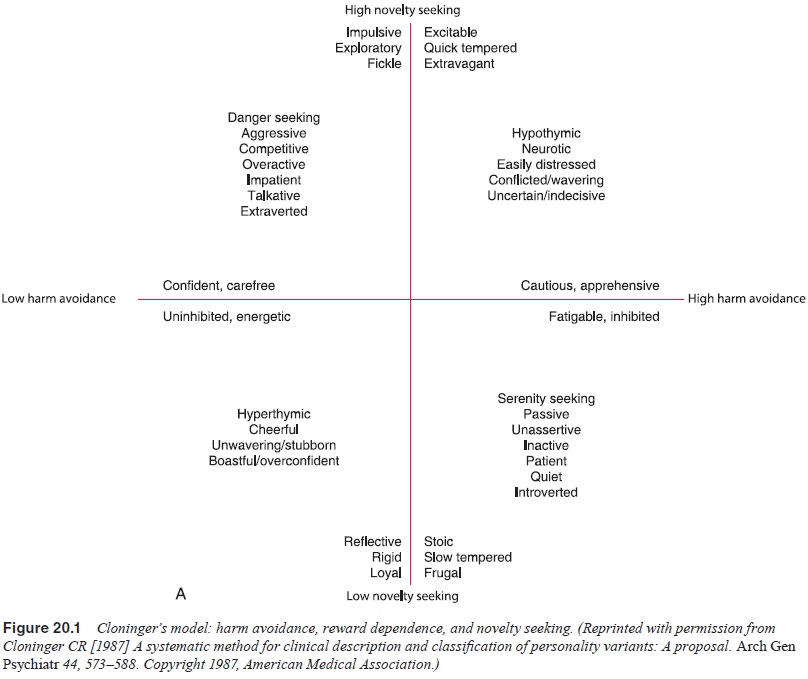
These four dimensions include novelty seeking, harm
avoidance, reward dependence and persistence. Figure 20.1 is a schematic
representation of Cloninger’s model.
Cloninger also describes three dimensions of
character, namely, self-directedness, cooperativeness, and self-transcen-dence.
The blend of these three characteristics that an individual possesses helps to
determine self-concept, such as whether the individual identifies himself or
herself as an autonomous individ-ual, as an integral part of humanity, and as a
part of the universe as a whole. Those with low degrees of self-directedness
and low degrees of cooperativeness are more likely to have personality
disorders (Svrakic et al., 1993).
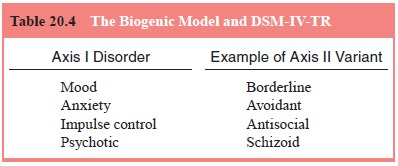
A third dimensional model of personality is the
biogenic spectrum model of Siever and Davis (1991). This model pro-poses that
certain personality styles and disorders are associ-ated with and are
characterological variants of various Axis I disorders. Thus, personality
disorders are not extreme variants of normal but are characterological variants
of Axis I disor-ders. The biogenic spectrum model may be useful in guiding
treatment, such as using anxiolytics to treat avoidant personal-ity disorder
because it is considered to be on a spectrum with Axis I anxiety disorders.
There is growing evidence that the biogenic spectrum model is useful for at
least some Axis I/Axis II disorders. One example is the link between
schizophrenia and schizotypal personality disorder in which those with the Axis
II disorder demonstrate a better capacity for buffering in certain frontal
brain regions as shown by functional imaging as compared with those with the
full-blown Axis I disorder (Kir-rane and Siever, 2000). Table 20.4 presents details
of the bio-genic model
Related Topics