Chapter: Paediatrics: Special senses
Paediatrics: Squints (strabismus)
Squints (strabismus)
Squints are common in childhood.
They occur with misalignment of the visual axes of the two eyes so that they
appear to point in different direc-tions. If a squint develops in the first
7yrs, it can have a significant impact on visual development.
The causes of squint may be:
•
Idiopathic.
•
Refractive
error.
•
Visual
loss.
•
Ophthalmoplegia
(central or peripheral).
Types of squint
There are two main types.
Concomitant (non-paralytic) squint
•
Common
and usually due to a refractive error in one or both eyes.
•
Often
convergent.
Non-concomitant (paralytic) squint
•
Rare
and usually due to cranial (motor) nerve palsy.
•
Must
exclude an intracranial lesion (e.g. brain tumour).
Describing squints
Squints are described using the
following terminology.
•
Convergent: bad eye turned inwards (cross-eyed
appearance)
•
Divergent: bad eye turned outwards
•
Latent: a squint that is controlled by
subconscious effort and is not always
apparent. In certain situations, such as fatigue, the control is lost and the
squint will become ‘manifest’
•
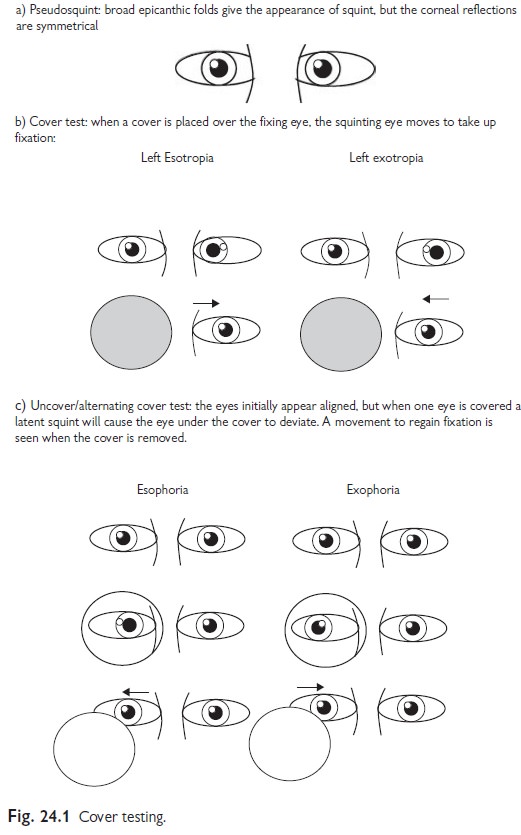
Pseudosquint: this arises when wide epicanthic
folds give the appearance of a
squint, which is excluded on testing
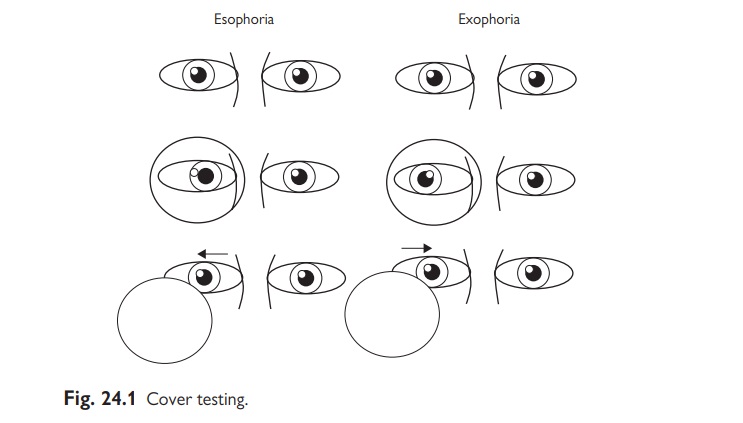
Testing squints
All squints should
be examined using the ‘cover test’ (see Fig. 24.1).
Management
The aim of treatment is to get the
‘weaker’ squinting eye ‘trained up’ in order to prevent amblyopia. Treatments
are usually under the supervision of orthoptists in co-operation with
ophthalmic surgeons.
•
Correct refractive error: wear glasses.
•
Eye
patch wearing on the good eye to ‘train’ weaker eye.
•
Eye
muscle exercises.
•
Eye (muscle)
surgery if large squint and above measures failing.
Note:
A child must be seen by an
ophthalmologist if squint is:
•
Divergent
•
Paralytic
•
Persistent
beyond age of 2mths
Related Topics