Chapter: Paediatrics: Gastroenterology and nutrition
Paediatrics: Nutritional disorders
Nutritional disorders
Malnutrition is a common cause of
child mortality and morbidity. There is a wide spectrum of nutritional
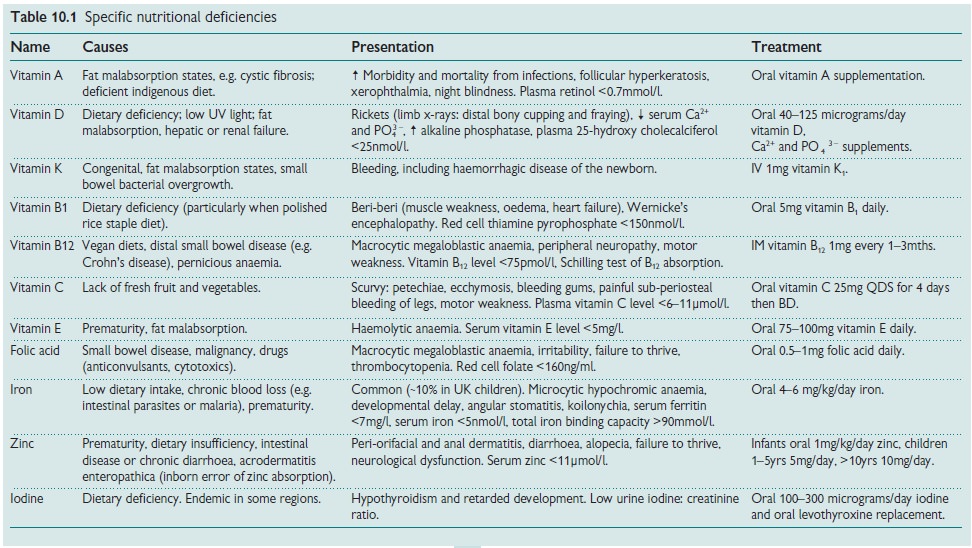
disorders, varying from protein-energy malnutrition to micronutrient nutritional
deficiencies to morbid obesity (see Table 10.1). In non-industrialized nations
malnutrition and associated infection are leading causes of child death.
Causes
ŌĆó
Diets
low in protein, energy, or specific nutrients.
ŌĆó
Strict
fad or vegetarian diets.
ŌĆó
Diseases
causing malabsorption (e.g. coeliac disease, cystic fibrosis, CrohnŌĆÖs disease),
severe GORD, immunodeficiency, chronic infection.
ŌĆó
Eating
disorders, e.g. anorexia nervosa.
Assessment of nutritional status
Refer to a paediatric dietician
and review the following:
┬Ę Recent weight loss ( 10% over
3mths is suggestive of impaired nutritional status).
ŌĆó
Accurately
plot serial height and weight (falling across 2 centile lines or below 3rd
centile may indicate nutritional impairment).
ŌĆó
Percentage
weight for height (= [actual weight/expected weight for height centile] x 100); a value of 90% may indicate
impairment.
ŌĆó Body mass index (BMI) = weight
(kg)/height (m)2.
ŌĆó Mid-arm circumference divided by
head circumference (malnutrition if <0.31).
ŌĆó
Detailed
dietary assessment of 5ŌĆō7-day food diary.
ŌĆó Serum albumin.
ProteinŌĆōenergy malnutrition
Kwashiorkor and marasmus usually
occur together. Because of oedema, mid-upper arm circumference is a better
guide to malnutrition than weight. Kwashiorkor
is due to severe deficiency of protein/essential amino acids.
┬Ę Clinical
features: growth
retardation; diarrhoea; apathy; anorexia;
ŌĆó
oedema;
skin/hair depigmentation; abdominal distension with fatty
┬Ę liver.
ŌĆó
Investigations: hypoalbuniaemia, normo- and
microcytic anaemia, ŌĆśfallŌĆÖ Ca2+,
ŌĆśfallŌĆÖ Mg2+, ŌĆśfallŌĆÖ PO34ŌĆō , and
ŌĆśfallŌĆÖ glucose.
ŌĆó
Marasmus: is due to severe energy (calories)
deficiency.
ŌĆó
Clinical features: height is relatively preserved
compared to weight; wasted
appearance; muscle atrophy; listless; diarrhoea; constipation.
ŌĆó
Investigations: ŌĆśfallŌĆÖ Serum albumin, Hb, U&E, Ca2+,
Mg2+, PO43 ŌĆō, and glucose; stool M,C&S for intestinal ova, cysts, and parasites.
Treatment
ŌĆó
Correct
dehydration and electrolyte imbalance (IV if required).
ŌĆó
Treat
underlying infection and/or parasitic infections.
ŌĆó
Treat
concurrent/causative disease.
ŌĆó
Treat
specific nutritional deficiencies.
ŌĆó Orally refeed slowly- watch out for refeeding syndrome.
Related Topics