Chapter: Nutrition and Diet Therapy: The Relationship of Nutrition and Health
Nutrition Assessment
NUTRITION ASSESSMENT
That old saying, “You
are what you eat,” is true, indeed; but one could change it a bit to read, “You
are and will be what you eat.” Good
nutrition is essential for the attainment and maintenance of good health.
Determining whether a person is at risk requires completion of a nutrition assessment, which should, in
fact, become part of a routine exam done by a registered dietitian or other health care
professional specifically trained in thediagnosis of at-risk individuals. A
proper nutrition assessment includes anthropometric
measurements, clinical examination, biochemical tests, and dietary-social history.
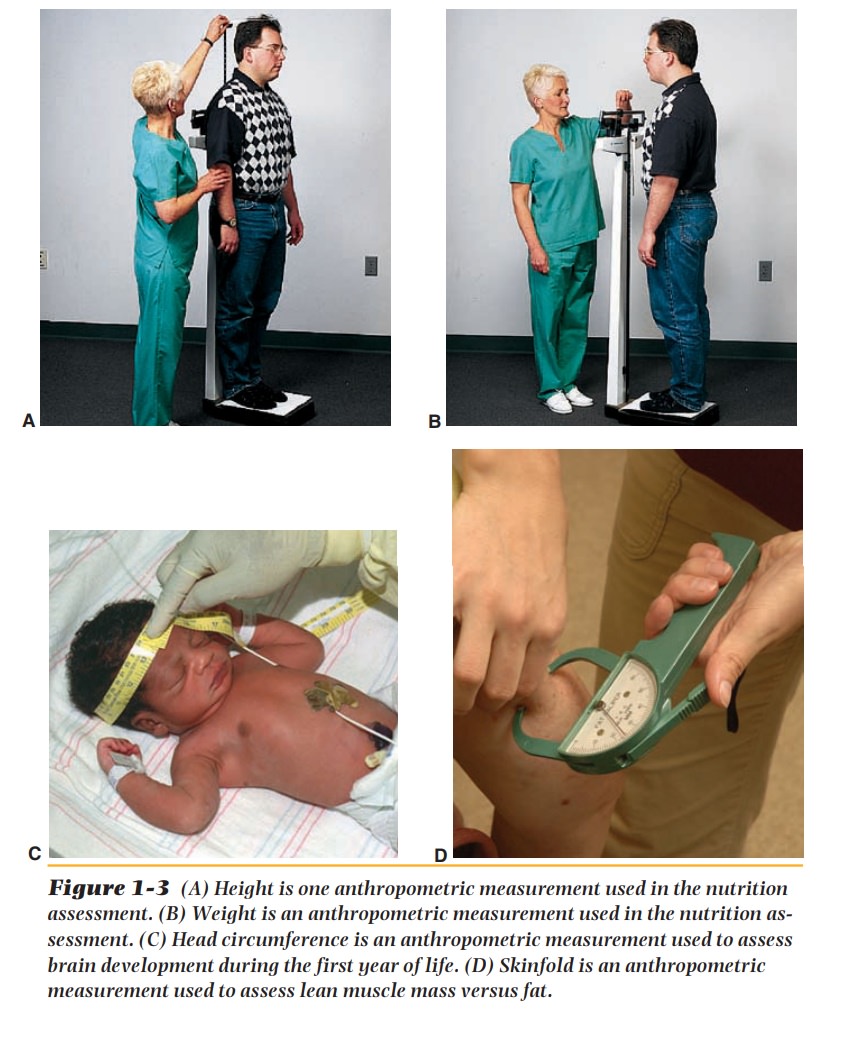
Anthropometric
measurements include height and weight and measure-ments of the head (for
children), upper arm, and skinfold (Figure 1-3). The skinfold measurements are
done with a caliper. They are used to
determine the percentage of adipose and muscle tissue in the body. Measurements
out of line with expectations may reveal failure to thrive in children, wasting
(catabo-lism), edema, or obesity, all of which reflect nutrient deficiencies or
excesses.
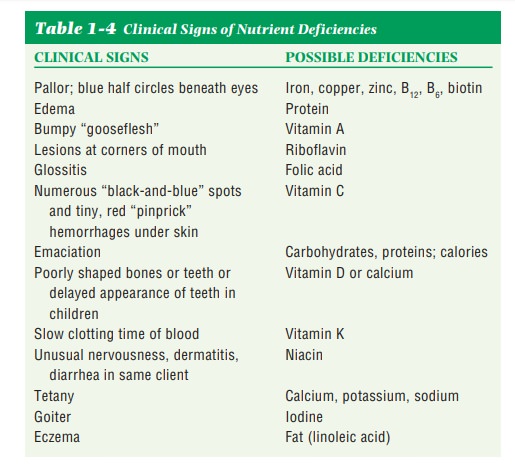
During the clinical examination, signs of nutrient deficiencies are noted. Some nutrient deficiency diseases, such as scurvy, rickets, iron deficiency, and kwashiorkor, are obvious; other forms of nutrient deficiency can be far more subtle. Table 1-4 lists some clinical signs and probable causes of nutrient defi-ciencies.
Biochemical tests
include various blood, urine, and stool tests. A defi-ciency or toxicity can be
determined by laboratory analysis of the samples. The tests allow detection of
malnutrition before signs appear. The following are some of the most commonly
used tests for nutritional evaluation.
· Serum albumin level measures the main
protein in the blood and isused to determine protein status.
· Serum transferrin level indicates
iron-carrying protein in the blood.The level will be above normal if iron
stores are low and below normal if the body lacks protein.
· Blood urea nitrogen (BUN) may indicate
renal failure, insufficient re-nal blood supply, or blockage of the urinary
tract.
· Creatinine excretion indicates the amount
of creatinine excreted inthe urine over a 24-hour period and can be used in
estimating body muscle mass. If the muscle mass has been depleted, as in
malnutrition, the level will be low.
· Serum creatinine indicates the amount
of creatinine in the blood andis used for evaluating renal function.
Examples of other
blood tests are hemoglobin (Hgb), hematocrit (Hct), red blood cells (RBCs), and
white blood cells (WBCs). A low Hgb and Hct can indicate anemia. Not a routine
test, but ordered on many clients with heart conditions, is the lipid profile,
which includes total serum cholesterol, high-density lipoprotein (HDL),
low-density lipoprotein (LDL), and serum triglycerides. Urinalysis also can
detect protein and sugar in the urine, which can indicate kidney disease and
diabetes.
The dietary-social
history involves evaluation of food habits and is very im-portant in the
nutritional assessment of any client. It can be difficult to obtain an accurate
dietary assessment. The most common method is the 24-hour
recall. In this method, the client is usually interviewed by the
dietitian and is asked to give the types of, amounts of, and preparation used
for all food eaten in the 24 hours prior to admission (PTA). Another method is
the food diary. The client is asked
to list all food eaten in a 3–4-day period. Neither method is totally accurate
because clients forget or are not always totally truthful. They are sometimes
inclined to say they have eaten certain foods because they know they should
have done so. Computer analysis of the diet is the best way to determine if
nutrient intake is ap-propriate. It will reveal any nutrient deficiencies or
toxicities.
The dietary-social
history is important to determine whether the client has the financial
resources to obtain the needed food and the ability to properly store and cook
food once home. After completing the dietary-social history, the dietitian can
assess for risk of food–drug interactions that can lead to malnutri-tion (see
Appendix E). Clients need to be instructed by a dietitian on possible
interactions, if any.
When the preceding
steps are evaluated together, and in the context of the client’s medical
condition, the dietitian has the best opportunity of making an accurate
nutrition assessment of the client. This assessment can then be used by the
entire health care team. The doctor will find it helpful in evaluating the
client’s condition and treatment. The dietitian can use the information to plan
the client’s dietary treatment and counseling, and other health care
pro-fessionals will be able to use it in assisting and counseling the client.
Related Topics