Chapter: Ophthalmology: Lacrimal System
Lacrimal System: Examination Methods
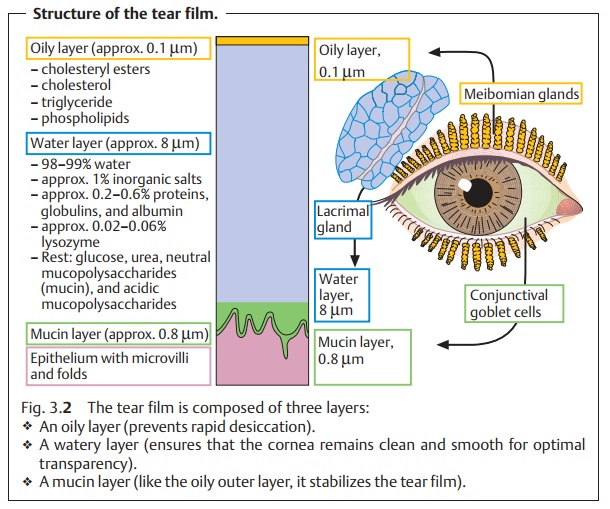
Examination Methods
Evaluation of Tear Formation
Schirmer tear testing: This test (Fig. 3.4)
provides information on thequan-tity of
watery component in tear secretion.
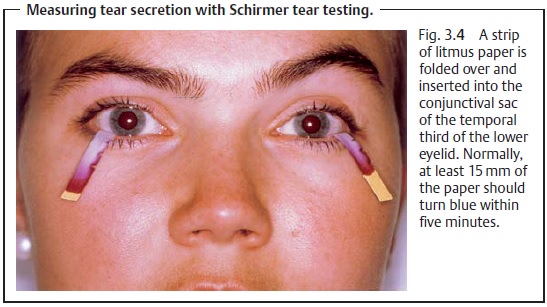
❖ Test: A strip of litmus paper is inserted into the
conjunctival sac of the tem-poral third of the lower eyelid.
❖ Normal: After about five minutes, at least 15 mm of
the paper should turnblue due to the alkaline tear fluid.
❖ Abnormal: Values less than 5 mm are abnormal (although
they will notnecessarily be associated with clinical symptoms).
The same method is used after application of a
topical anesthetic to evaluate normal secretion without
irritating the conjunctiva.
Tear break-up time (TBUT): This test evaluates thestability
of the tear film.
❖ Test: Fluorescein dye (10µl of a 0.125%
fluorescein solution) is added to theprecorneal tear film. The examiner
observes the eye under 10 – 20 power magnification with slit lamp and cobalt
blue filter and notes when the first signs of drying occur (i) without the patient closing the eye and
(ii) with the patient keeping the eye
open as he or she would normally.
❖ Normal: TBUT of at least 10 seconds
is normal.
Rose bengal test: Rose bengaldyes dead epithelial cells and mucin.This testhas proven particularly useful in evaluating dry eyes (keratoconjunctivitis sicca) as it reveals conjunctival and corneal symptoms of desiccation.
Impression cytology: A Millipore filter is fastened to a tonometer andpressed against
the superior conjunctiva with 20 – 30 mm Hg of pressure for two seconds. The density of goblet cells is estimated
under a microscope (normal density is
20 – 45 goblet cells per square millimeter of epithelial sur-face). The number
of mucus-producing goblet cells is reduced in various dis-orders such as
keratoconjunctivitis sicca, ocular pemphigoid, and xeroph-thalmia.
Evaluation of Tear Drainage
Conjunctival fluorescein dye test: Normaltear drainagecan
be demon-strated by having the patient blow his or her nose into a facial
tissue following application of a 2% fluorescein sodium solution to the
inferior fornix.
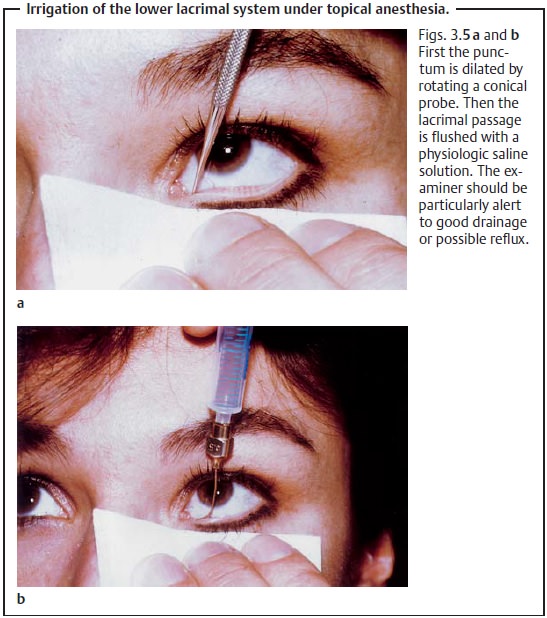
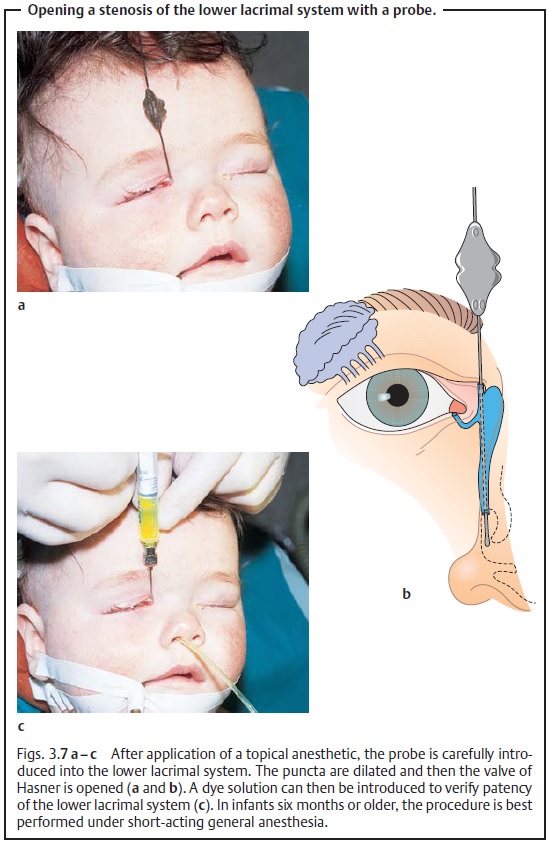
Probing and irrigation: These examination methods are used tolocate ste-noses. After application of a topical anesthetic, a
conical probe is used todilate the punctum. Then the lower lacrimal system is
flushed with a physio-logic saline solution introduced through a blunt cannula
(Figs. 3.5 a andb). If the passage is unobstructed,
the solution will drain freely into the nose.
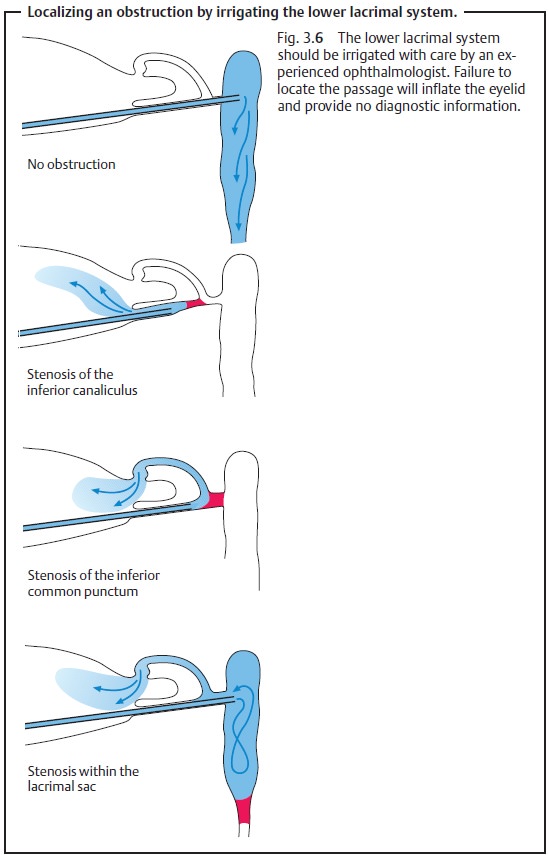
Canalicular stenosis will result in reflux
through the irrigated punctum. If the stenosis is deeper, reflux will occur
through the opposite punctum (Fig. 3.6).
A probe can be used to determine the site of
the stricture, and possibly to eliminate obstructions (Fig. 3.7).
Radiographic contrast studies: Radiographic contrast medium is instilled inthe same manner as
the saline solution. These studies demonstrate the shape, position, and size of the passage and possible obstructions to drainage.
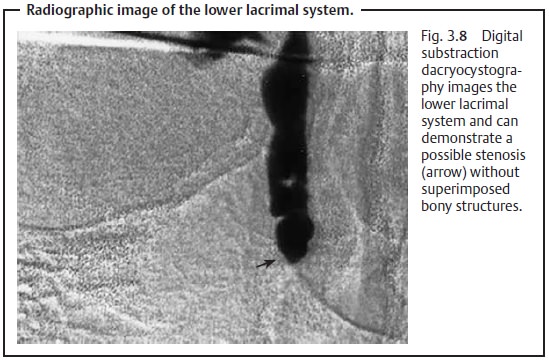
Digital substraction dacryocystography: These studies demonstrate onlythe contrast medium and image the lower lacrimal system without superim-posed bony structures. They are particularly useful as preoperative diagnostic studies (Fig. 3.8).
Lacrimal endoscopy: Fine endoscopes now permit direct
visualization ofthe mucous membrane of the lower lacrimal system. Until
recently, endo-scopic examination of the lower lacrimal system was not a
routine procedure.
Related Topics