Chapter: Modern Pharmacology with Clinical Applications: Immunomodulating Drugs
Individual Drugs Used to Stimulate the Immune System
INDIVIDUAL DRUGS
USED TO STIMULATE THE IMMUNE SYSTEM
A number of disorders can be
treated with immuno-stimulating agents (also
known as biological response modifiers
or immunomodulating agents); these drugs enhance the body’s immune response.
These conditions include immunodeficiency diseases, cancer, some types of viral
and fungal infections, and certain autoimmune disorders. The drugs may work on
cellular or humoral immune systems or both.
Immunostimulating agents are
nonspecific; they cause general stimulation of the immune system. Among the
agents capable of general potentiation of the immune sys-tem are extracts and
derivatives from bacteria, yeast, and fungi. They also include a variety of
peptides, cytokines, and synthetic compounds. In most cases, the pharmacol-ogy
of these agents has not been well described. The most commonly used agents are
discussed next.
Bacillus Calmette-Guérin
Bacillus Calmette-Guérin
(BCG) is a viable attenuated strain of Mycobacterium
bovis. Nonviable strains of the bacterium also have been shown to augment
the im-mune response. The smallest active compound derived from BCG thus far
has been identified as muramyl dipeptide. The T cell is a principal target for
BCG. It also appears to stimulate natural killer cells, which in turn can kill
malignant cells. It has been suggested that BCG cross-reacts immunologically
with tumor cell antigens.
BCG immunotherapy has been
most successful in the treatment of bladder cancers. It is instilled directly
into the bladder, where it is held for 2 hours before urination.
The most dangerous
complications of BCG therapy are severe hypersensitivity and shock. Chills,
fever, malaise, immune complex, and renal disease are among the other side
effects. The route of administration influ-ences the nature of the side
effects.
Levamisole
Levamisole (Ergamisol) was originally developed as
an antihelminthic drug . It potentiates the stimulatory effects of antigens,
mitogens, lymphokines, and chemotactic factors on lymphocytes, granulocytes,
and macrophages. It has been shown to increase T cell–mediated immunity.
Levamisole has been used
successfully in treating chronic infections. It also has been approved for use
in combination with fluorouracil in the treatment of col-orectal cancer.
Immune Globulin
Immune globulin is isolated
from pooled human plasma either from donors in the general population or from
hyperimmunized donors. It is used principally in the treatment of certain
immune deficiencies. Standard im-mune globulin solutions contain a distribution
of all subclasses, with antibody titers for most major bacterial, viral, and
fungal pathogens.
Immune globulin, given
intramuscularly or intra-venously, is recommended in the treatment of primary
humoral immunodeficiency, congenital agammaglobu-linemias, common variable
immunodeficiency, severe combined immunodeficiency, idiopathic
thrombocy-topenic purpura, and autoimmune hemolytic anemia. There are six
licensed preparations of immune globulin.
The principal side effects
are possible anaphylactoid reactions and severe hypotension.
Thymic Factors
Thymic factors are naturally
occurring substances that promote T-lymphocyte differentiation and
differentia-tion of early stem cells into prothymocytes. Each of the available
preparations (e.g., thymic humoral factor, thy-mosin fraction 5, and
thymodulin) are mixtures of sev-eral polypeptides isolated from a calf thymus
extract.
By promoting the formation of
T lymphocytes, thymic factors are used to enhance T-lymphocytic func-tions.
Thymic factors have been used with some success in clinical trials in patients
with severe combined im-munodeficiency, DiGeorge’s or Nezelof’s syndrome, and
viral disorders. Studies with thymodulin show promise in treating symptoms in
asthmatics and pa-tients with allergic rhinitis. The primary consideration in
the use of thymic factors for immunodeficiency states is the presence of
T-lymphocyte precursors.
Few major side effects have
been reported, espe-cially with purer forms produced by genetic engineer-ing.
Crude thymic preparations have produced allergic side effects in some patients.
Cytokines
An exciting application of
immunomodulating therapy is in the use of cytokines (lymphokines, monokines). As mentioned earlier, immune cell function
is regulated by cytokines produced by leukocytes or other supporting cells.
With the advent of genetic engi-neering, cytokines can be produced in pure form
and in large quantities.
Interleukin-2
IL-2 (Proleukin) is a cytokine that promotes the prolif-eration,
differentiation, and recruitment of T and B lym-phocytes, natural killer cells,
and thymocytes. Human recombinant IL-2 is designated as rIL-2. rIL-2 binds to
IL-2 receptors on responsive cells and induces prolifer-ation and
differentiation of T helper cells and T cyto-toxic cells. It also can induce
B-lymphocyte prolifera-tion, activate macrophage activity, and augment the
cytotoxicity of natural killer cells.
rIL-2 is administered
systemically as an immunos-timulating agent in patients with AIDS and to
augment specific antitumor immunity. Patients with renal cell carcinoma or
melanoma have been effectively treated with rIL-2 in combination with adoptive
transfer im-munotherapy. The latter refers to the injection of the patient’s
own cytokine-activated killer cells or tumor-infiltrating lymphocytes after
they reside in tissue cul-ture for several weeks in the presence of rIL-2.
Systemic administration of
rIL-2 causes fever, nau-sea, vomiting, fatigue, and malaise. Other adverse
af-fects include flushing, diarrhea, chills, rash, edema, symptomatic
hypotension, and certain renal abnormali-ties. These tend to occur at increased
dosage levels and are attenuated by reducing the dosage.
Myeloid Colony–Stimulating Factors
Recombinant
granulocyte-macrophage colony–stimu-lating factor (GM-CSF) (Sargramostim) and granulo-cyte
stimulating factor (G-CSF) (Filgrastim)
are cy-tokines, or growth factors, that support the survival, clonal expansion,
and differentiation of hematopoietic cells. These factors are normally produced
in the body by monocytes, fibroblasts, and endothelial cells. GM-CSF induces
bone marrow progenitor cells belonging to the granulocyte or macrophage lineage
to divide and differentiate into mature cells. G-CSF induces the mat-uration of
granulocyte progenitor cells.
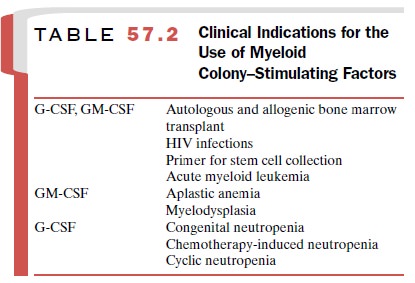
In general these recombinant
cytokines are indi-cated for acceleration of the recovery of circulating white
blood cells in patients who have depressed hematopoiesis, as a result of either
chemotherapy or congential disorders of hematopoiesis. A list of indica-tions
for the use of GM-CSF and G-CSF is provided in Table 57.2.
Results of several phase 1 and phase 2 clinical trials suggest that these cytokines are well tolerated. Adverse effects are those commonly observed following the ad-ministration of molecules produced by biotechnological means.
They include diarrhea,
asthenia, rash, malaise, fever, headache, bone pain, chills, and myalgia. Many
of these effects can be ameliorated by the administration of analgesics and
antipyretics.
Other Cytokines
Human recombinant interferon-
(rIFN- ) and rIL-1 also show promise as immunostimulators, principally as
adjuvants in the treatment of viral and malignant disor-ders.
rIFN- is produced by
leukocytes and inhibits viral DNA and RNA replication. At lower doses, it can
stim-ulate macrophages, T lymphocytes, and natural killer cell activity.
rIL-1 is produced by
macrophages in the host and is necessary for activation and development of
immune cells. Intravenous administration of rIL-1 is associated with the
general augmentation of immune responses.
rIL-6 is a protein that
stimulates lymphocyte and megakaryocyte proliferation. It is in clinical trials
in pa-tients with refractory cancer and myelodysplastic syn-drome. Trials also
are ongoing with rIL-3, a multipotent factor that stimulates the growth of
monocytes, erythro-cytes, neutrophils, and megakaryocytes.
Related Topics