Chapter: Essentials of Psychiatry: Impulse Control Disorders
Impulse Control Disorders
Impulse Control Disorders
The trait
of impulsivity has been the subject of increasing in-terest in psychiatry. New
research findings seem to associate various forms of impulsive behavior with
biological markers of altered sero-tonergic function. These include impulsive
suicidal behavior, impul-sive aggression and impulsive fire-setting.
Impulsivity is also a focus of interest in the increasing attention paid to the
behavioral phenome-nology of borderline personality disorder. In all these
circumstances, impulsivity is conceived of as the rapid expression of unplanned
be-havior, occurring in response to a sudden thought. (This is seen by some as
the polar opposite of obsessional behavior, in which delibera-tion over an act
may seem never-ending.) Although the sudden and unplanned aspect of the
behavior may be present in the impulse dis-orders (such as in intermittent
explosive disorder and kleptomania), the primary connotation of the word
impulsivity, as used to describe these conditions, is the irresistibility of
the urge to act.
The
National Comorbidity Survey Replication (NCS-R) (Kessler et al., 2005) extended the definition of impulse control disorders
described to include intermittent explo-sive disorder, attention deficit
hyperactivity disorder (ADHD), conduct disorder (CD) and oppositional defiant
disorder (ODD). This decision was based on the fact that ADHD and anger
symp-toms often persist throughout adulthood. The NCS-R found that the combined
lifetime prevalence for these disorders is greater than that of mood (20.8%) or
substance abuse disorders (14.6%). Impulse control disorders in the extended
definition had a 12 month prevalence of 8.9% and a lifetime prevalence of
24.8%. Moreover, this group was judged to have a greater proportion functioning
at the serious level than either anxiety or substance abuse disor-ders. with
approximately half of all lifetime cases receiving no treatment. An important
objective in studying the impulse control disorders in this fashion was to
highlight how common hostility and aggression are in psychiatric disorders, two
dimensions often not receiving sufficient diagnostic consideration but which
are significantly present as comorbidities with other disorders.
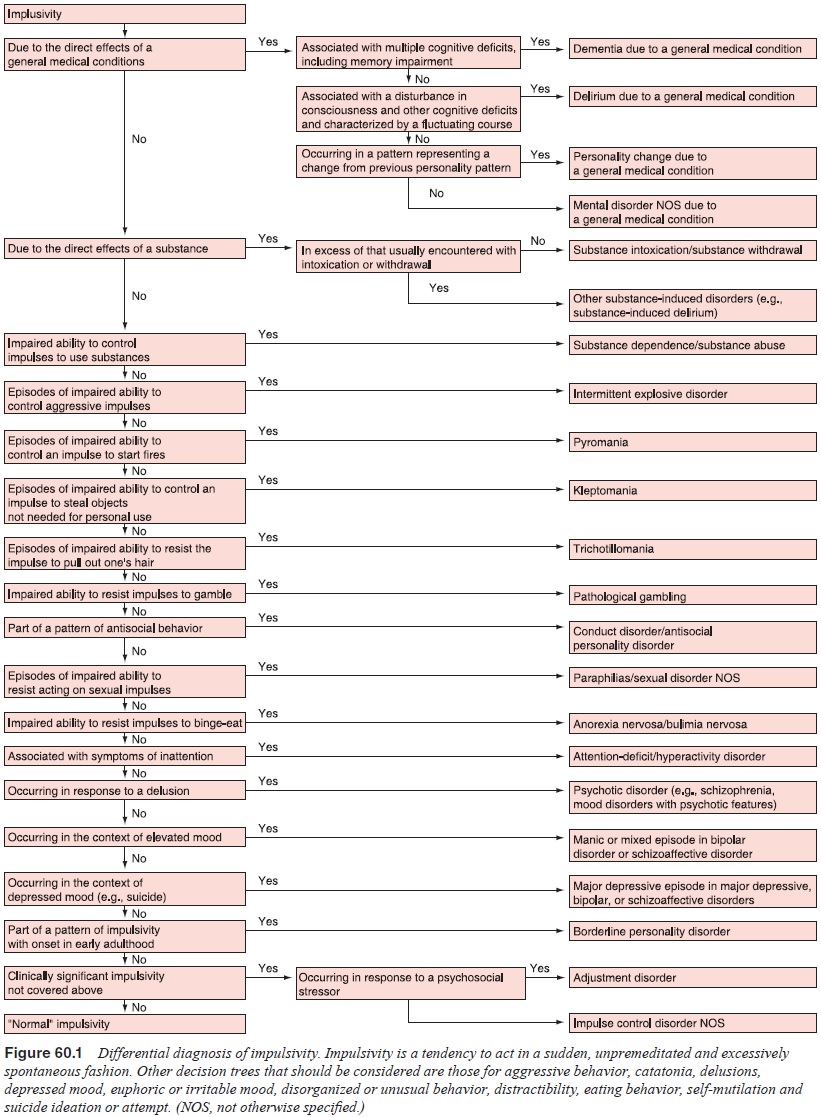
Trichotillomania,
pyromania and pathological gambling may involve episodes in which a sudden
desire to commit the act of hair-pulling, fire-setting, or gambling is followed
by rapid expression of the behavior. But in these conditions, the individual
may spend considerable amounts of time fighting off the urge, trying not to
carry out the impulse. The inability to resist the impulse is the common core
of these disorders, rather than the rapid transduction of thought to action. A
decision tree for the differen-tial diagnosis of impulsive behaviors may be
seen in Figure 60.1.
Other
than sharing the essential feature of impulse dyscon-trol, it is unclear
whether the conditions bear any re-lationship to each other. Emerging
perspectives on the neurobiology of impulsivity suggest that impulsive
behaviors, across diagnostic boundaries, may share an underlying
pathophysiological diathesis. As noted earlier, markers of altered serotonergic
neurotransmission have been associated with a variety of impulsive behaviors:
suicid-ality, aggressive violence, pyromania and conduct disorder. These
observations have led to speculation that decreased serotonergic
neurotransmission may result in decreased ability to control urges to act. In
accord with this model, these disorders may be varying expressions of a single
disturbance – or closely related disturbances – of serotonergic function.
Although such markers of altered sero-tonergic function have been demonstrated
among impulsive fire-setters and impulsive violent offenders, there is, as yet,
insufficient research on these conditions to accept or dismiss this theory.
It has
been noted that these conditions are embedded in similar patterns of
comorbidity with other psychiatric disorders. High rates of comorbid mood
disorder and anxiety disorder ap-pear typical of these disorders. This
contextual similarity, com-bined with the common feature of impulsivity, may
further sup-port the notion that these conditions are – at the level of core
diathesis – related to each other.
Although
these conditions have historically been consid-ered uncommon, later
investigations suggest that some of them may be fairly common.
Trichotillomania, for example, was once considered rare. However, surveys
indicate that the lifetime prev-alence of the condition may exceed 1% of the
population. Patho-logical gambling may be present in up to 3% of the
population. Extrapolation from the known incidence of comorbid conditions
suggests that kleptomania may have a 0.6% incidence. It would seem reasonable
to suspect that individuals with pyromania and kleptomania may seek to avoid
detection and may therefore be underrepresented in research and clinical
samples.
Treatment
protocols for these conditions have not been well studied. Few treatment
studies of these specific conditions have been performed. Attempts to treat
these conditions are usu-ally formulated by extrapolation from treatments that
have been developed for other conditions.
The aggressive quality of kleptomania, pyromania and intermittent explosive disorder and the self-damaging nature of trichotillomania and pathological gambling have presented tempting substrates for the application of traditional analytical concepts. From this perspective, these behaviors have been seen as symptomatic expressions of unconscious conflict, often sexual in nature. Other formulations include desires for oral gratification and masochistic wishes to be caught and punished, motivated by a harsh, guilt-inducing superego. The increasing influence of object relations theory was reflected in increasing emphasis on narcissistic psychopathology and histories of disturbed early par-enting. As successful behavioral interventions were developed for other conditions, case reports of behavioral treatments for these conditions emerged. Reports of hypnotic treatments are also prominent in the literature.
The
contemporary medical and psychological literature reflects, not surprisingly,
prevailing general interests in current research and theory. As pharmacological
treatments are applied to an increasing range of symptoms, the impulse
disorders present new opportunities to widen the application of thymoleptic and
anxiolytic and, more recently, (atypical) neuro-leptic medication. Some are
reconceptualizing the idea of mood and obsessional disorders, widening them
into affective and ob-sessional spectrums, encompassing various impulse
disorders into these domains.
As part
of the ongoing dynamic of evolving theory, the very concept of impulsivity is
still in ferment. Attempts further to refine the idea of impulsivity are
reflected in a perspective of-fered by Van Ameringen and associates (1999). In
a discussion of preliminary evidence indicating that trichotillomania may be
preferentially responsive to neuroleptics, they suggest that indi-viduals with
trichotillomania may have features in common with the subgroup of obsessive
compulsive disorder (OCD) patients who have comorbid Tourette’s syndrome (TS).
These authors offer a thoughtful model, applying the idea of an “Impulsion”
(Shapiro and Shapiro, 1992), an action performed until a sense of “rightness”
is achieved, rather than a compulsion, which is de-signed to reduce an anxiety
brought on by an obsession. They go on to note one formulation of OCD, which
divides symptoms into three types: symmetry/hoarding, pure obsessions and contamina-tion/cleaning.
The symmetry/hoarding factor – impulsion-driven behavior – was differentially
related to OCD with comorbid TS. They point to recent data suggesting that the
OCD/TS subgroup is not as responsive to SSRI medication alone as other OCD sub-types,
but responds better to SSRI/neuroleptic combinations. These observations, taken
together with their report of enhanced response of trichotillomania to
neuroleptics, is the basis for their argument that trichotillomania should be
seen as more similar to OCD/TS then OCD, more impulsion than compulsion. The
idea of anxiously seeking “rightness” is consistent with the clinical
experience of many individuals with trichotillomania and is a thoughtful
addition to the other attributes associated with impul-sivity: anxiety
reduction, irresistibility of action and rapidity of its execution.
Trichotillomania
provides an example of the convergence of current research techniques and
treatment perspectives. The absence of new psychodynamic formulations would
seem to re-flect not an abandonment of dynamic theory but an acceptance that
such models are most useful in understanding individual patients rather than
providing universal explanations for the symptom. Dynamic considerations may be
useful in trying to understand why particular circumstances may provoke
episodes of the problem behavior for a particular individual.
Not all
these conditions are, as yet, receiving significant attention.
Trichotillomania, intermittent explosive disorder andpathological gambling have
become the focus of increasing inter-est. Kleptomania and pyromania, however,
remain stepchildren of research. Perhaps the legal implications of these
behaviors and their entanglement with similar, but not impulsively motivated,
behaviors complicate the availability of sufficient cases to facili-tate
research.
Because
of the limited body of systematically collected data, the following sections
largely reflect accumulated clinical experience. Therefore, the practicing
psychiatrist should be par-ticularly careful to consider the exigencies of
individual patients in applying treatment recommendations.
Related Topics