Chapter: Pharmaceutical Biotechnology: Fundamentals and Applications : Monoclonal Antibodies in Solid Organ Transplantation
Immunologic Targets: Rational Development/ Use of Monoclonal Antibodies in Organ Transplant
IMMUNOLOGIC
TARGETS: RATIONAL DEVELOPMENT/ USE OF MONOCLONAL ANTIBODIES IN ORGAN TRANSPLANT
The rational use of monoclonal antibodies in trans-plantation is focused
on the prevention of host immune recognition of donor tissue. There are two
ways in which allograft tissue can be immediately impaired secondary to the
host immune response: complement-dependent antibody mediated cell lysis (antibody-mediated
rejection) and T-cell-mediated parenchymal destruction leading to localized
allograft inflammation and arteritis (cellular-mediated rejec-tion) (Halloran,
2004). Pre-transplant screening for antibodies against donor tissues has
significantly reduced the incidence and severity of antibody-mediated
rejection. However, as will be discussed, preferential destruction of cells
that produce these antibodies using monoclonal technology, such as rituximab,
prior to transplant has become an option for recipients with preformed
alloantibodies. Prevention and treatment of cellular-mediated rejec-tion,
therefore, is the main focus of maintenance immunosuppression and the rationale
for use of monoclonal antibodies in the early post-transplant period. Cellular
mediated rejection is characterized by initial recognition of donor tissue by
T-cells. This leads to a complex signal transduction pathway tradition-ally
described as three signals (Halloran, 2004):
· Signal 1: Donor antigens are
presented to T-cells leading to activation
·
Signal 2: CD80 and CD86 complex
with CD28 on the T-cell surface activating signal transduction pathways
(calcineurin, mitogen-activated protein kinase, protein kinase C, nuclear
factor kappa B) which leads to further T-cell activation, cytokinerelease and
expression of the interleukin-2 (IL-2) receptor (CD25)
·
Signal 3: IL-2 and other growth
factors cause the activation of the cell cycle and T-cell proliferation
(Halloran, 2004)
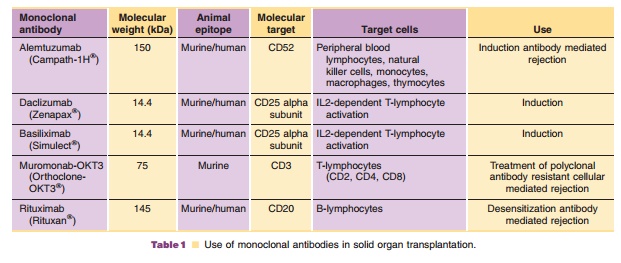
Monoclonal antibodies have been developed against various targets within
this pathway to prevent propagation and lymphocyte proliferation providing
profound immunosuppression (Table 1). Monoclonal antibodies that were
originally developed for treat-ment of various malignancies have also been
em-ployed as immunosuppressant agents in solid organ recipients. Use of these
agents must be balanced with maintenance immunosuppression to minimize the
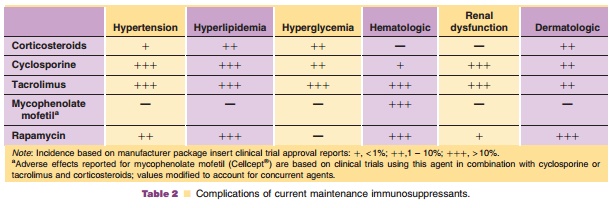
patient’s risk of infection or malignancy from over immunosuppression. Table 2
summarizes when and which monoclonal antibodies are currently used in solid
organ transplantation.
Related Topics