Chapter: Obstetrics and Gynecology: Human Sexuality
Human Sexual Response

HUMAN SEXUAL RESPONSE
In evaluating sexual problems, it
is useful to consider the mechanisms of sexual response in women. Sexual
function and dysfunction are perhaps the supreme exam-ples of a necessary
blending of mind and body. This inter-action is crucial to the understanding of
the assessment and management of sexual problems. The dualistic ap-proach
common to more traditional models of sexual response limits the understanding
of female sexuality inso-far as it suggests that dysfunction is either
psychologic or biologic or psychologic plus biologic. Newer approaches are more
holistic in their representations of female sexual response.
Traditional Model
The traditional Masters and
Johnson and Kaplan models of the human sexual response cycle are being replaced
by intimacy-based sexual response models that take other factors into
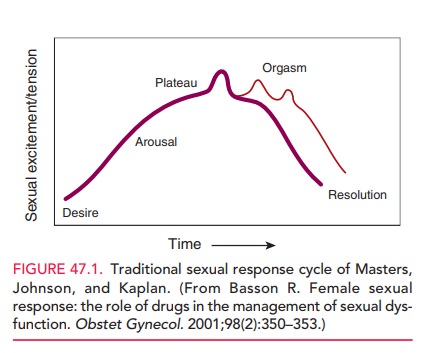
consideration. The traditional cycle depicts a linear sequence of events:
desire, arousal, plateau of constant high arousal, peak intensity arousal and
release (orgasm), possible repeated orgasms, and then resolution (Fig. 47.1).
However, the sexual response cycle in women is complex and events do not always
occur in a predictable sequence, as they usually do in men.
Neither the stimuli to which the
response occurs nor the nature of the “cyclicity” is evident in the traditional
model. The usefulness of this model for depicting women’s sexuality is limited
by the following considerations:
·
Women are sexual for many
reasons—sexual desire, as in sexual thinking and fantasizing, may be absent
initially.
·
Sexual stimuli are integral to
women’s sexual responses.
·
The phases of women’s desire and
arousal overlap.
·
Nongenital sensations and a
number of emotions frequently overshadow genital sensations in terms of
importance.
·
Arousal and orgasm are not
separate phenomena.
·
The intensity of arousal (even if
orgasm occurs) is highly variable from one occasion to another.
· Orgasm may not be necessary for satisfaction.
· The
outcome of the experience strongly influences the motivation to repeat it.
· Dysfunctions
may overlap (e.g., desire and arousal disorders, orgasm and arousal disorders).
Intimacy-based Model
An alternative sexual response
model depicts an intimacy-based motivation, integral sexual stimuli, and the
psycho-logical and biologic factors that govern the processing of those stimuli
(i.e., determining the woman’s arousability) (Fig. 47.2).
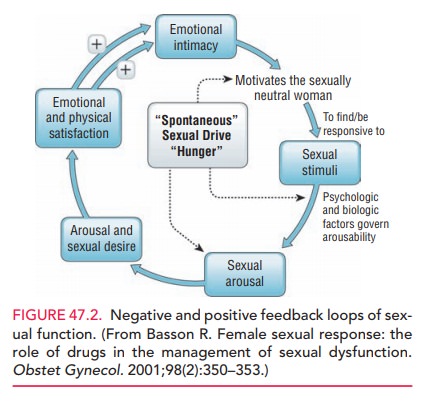
A woman’s primary motivation for
sexual response often is to be closer to her partner. If sexual arousal is
expe-rienced, the stimuli continue, the woman remains focused, and the sexual arousal
is enjoyed, she may then sense sexual desire to continue the experience for the
sake of the sexual sensations. A psychologic and physically positive outcome
heightens emotional intimacy with her partner, thereby strengthening the
motivation. Any spontaneous desire (i.e., sexual thinking, conscious sexual
wanting, and fantasiz-ing) may augment the intimacy-based cycle. Spontaneous
desire is particularly common early in relationships or when partners have been
apart, is sometimes related to the men-strual cycle, and is extremely variable
among women.
Physiology of Female Sexual Response
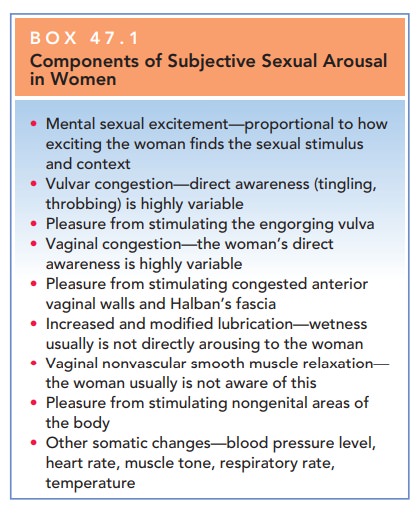
Systemically, the physiologic components of the female sexual response (Box 47.1) are mediated by increased activity of the autonomic nervous system and include tachy-cardia, skin flushing, and vaginal lubrication.
Box 47.1
Components of Subjective Sexual Arousal in Women
Mental sexual excitement—proportional to how exciting the woman finds
the sexual stimulus and context
Vulvar congestion—direct awareness (tingling, throbbing) is highly
variable
Pleasure from stimulating the engorging vulva
Vaginal congestion—the woman’s direct awareness is highly variable
Pleasure from stimulating congested anterior vaginal walls and Halban’s
fascia
Increased and modified lubrication—wetness usually is not directly
arousing to the woman
Vaginal nonvascular smooth muscle relaxation— the woman usually is not
aware of this
Pleasure from stimulating nongenital areas of the body
Other somatic changes—blood pressure level, heart rate, muscle tone,
respiratory rate, temperature
Several neuro-transmitters have been linked to the sexual response cycle. Norepinephrine, dopamine, oxytocin, and serotonin via 5-hydroxytriptamine 1A and 2C are
thought to have positive sexual effects; serotonin via most other receptors,
prolactin, and gamma-amino butyric acid are thought to affect the cycle
negatively.
Throbbing and tingling and
feelings of urgency for more genital contact and vaginal entry are far less
consis-tent for sexually healthy women than are the equivalent sensations in
men. Sexually healthy women typically expe-rience this confirmatory sexual
stimuli indirectly by the enjoyment of manual or oral stimulation or genital
stim-ulation with a vibrator, which are enhanced when there is vulvar
engorgement.
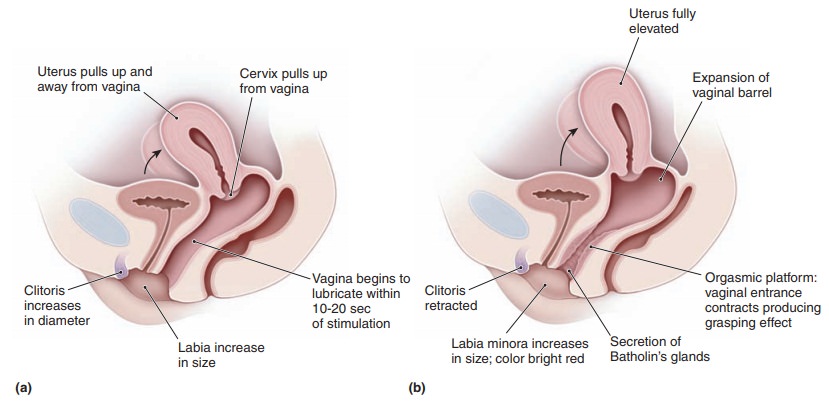
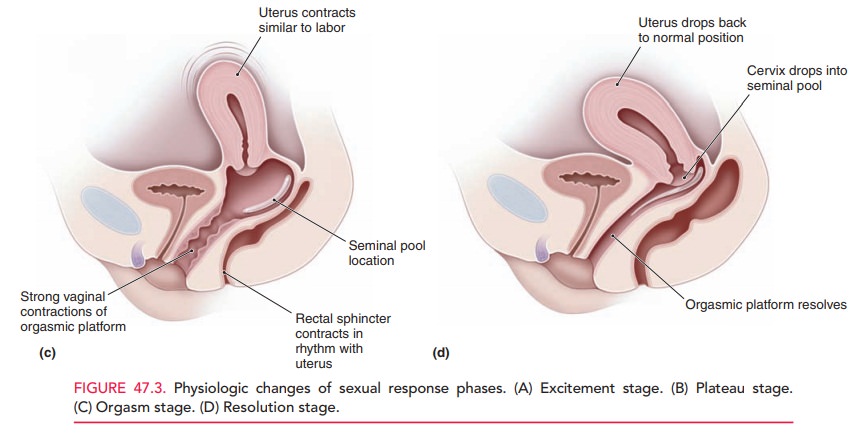
The measurement most commonly
used for vaginal congestion is the vaginal pulse amplitude. The upper por-tion
of the vagina dilates via a mechanism that is poorly understood. Figure 47.3
demonstrates some of the physio-logic changes seen in sexual response phases.
The duration of each phase varies with each individual and for a given
indi-vidual at different times in her life, and phases also can overlap.
Moreover, the state of subjective arousal is itself cognitively appraised.
Women consider the appropriateness of being sexual in a particular situation
and evaluate their safety. This moment-to-moment emotional and cognitive
feedback modulates the experience of arousal. The value of the phases depicted,
then, lies in their use in identifying the physiologic events that occur during
intimate encounters leading to climax. Clinically, the provider can inquire,
dur-ing the initial interview and in the course of ongoing ther-apy, about
whether or not these responses exist.
Related Topics