Chapter: Medical Surgical Nursing: Principles and Practices of Rehabilitation
Home and Community-Based Care - Rehabilitation
Home and Community-Based Care
An important goal of rehabilitation
is to assist the person to re-turn to the home environment after learning to
manage the dis-ability. A referral system maintains continuity of care when the
patient is transferred to the home or to an extended care facility. The plan
for discharge is formulated when the patient is first ad-mitted to the
hospital, and discharge plans are made with the pa-tient’s functional potential
in mind.
The patient’s support system (family, friends) is assessed. The attitudes of family and friends toward the patient, the disability, and the return home are important in making a successful tran-sition to home. Not all families are able to carry on the arduous programs of exercise, physical training, and personal care that a patient may need. They may not have the resources or stability to care for a severely disabled family member. Even a stable family may be overwhelmed by the physical, emotional, economic, and energy strains of a disabling condition in their family member. Members of the rehabilitation team must not judge the family but rather should provide supportive interventions that help them attain their highest level of function.
The family needs to know
as much as possible about the pa-tient’s condition and care so that they do not
fear the patient’s return home. The nurse develops methods for coping with
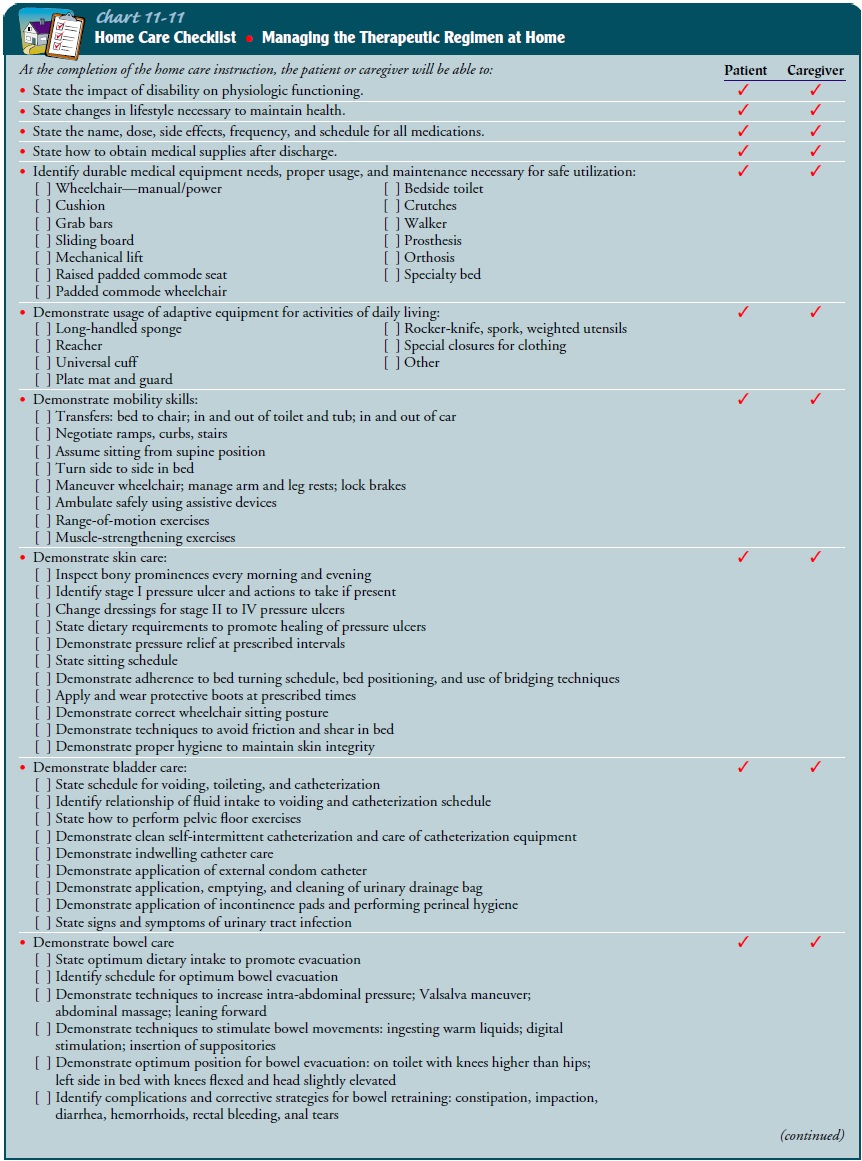
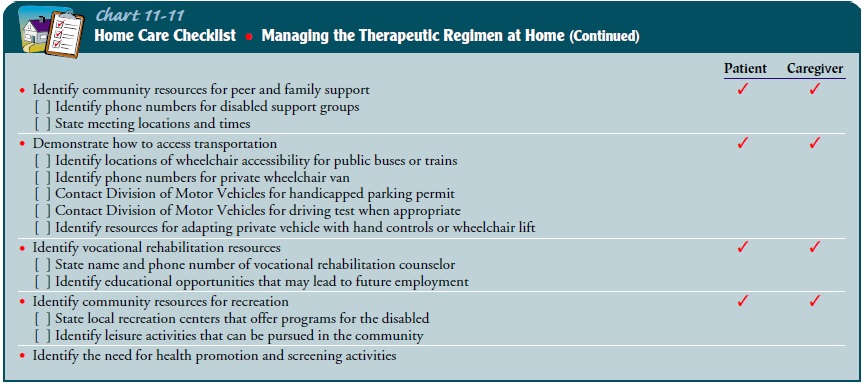
prob-lems that may arise with the patient and family. A skill checklist
individualized for the patient and family can be developed to make certain that
the family is proficient in assisting the patient with certain tasks. See Chart
11-11 for an example of a home care checklist.
Related Topics