Chapter: Essentials of Psychiatry: Stimulants and Related Compounds
Formulation of Treatment
Formulation
of Treatment
What Is Being Treated
There are two main indications for the use of MPH: narcolepsy and ADHD. Other stimulants differ somewhat, with the indica-tions for methamphetamine (Desoxyn Gradumets) including ADHD and obesity.
Diagnosis of the Stimulant-treatable Disorders
Attention-defi cit/Hyperactivity Disorder
ADHD is a
heterogeneous behavioral disorder of unknown etiol-ogy. As its name suggests,
ADHD is characterized by inattention, impulsivity and hyperactivity of varying
severity. The disorder, which typically begins in early childhood and lasts
into adult-hood in a substantial minority, if not a majority, of cases,
fre-quently leads to profound social and academic impairments. For a complete
discussion of the ADHD diagnosis, see Chapter 28.
Narcolepsy
Narcolepsy
is a chronic neurological disorder that presents with excessive daytime
sleepiness and various problems of rapid eye movement physiology, such as
cataplexy (unexpected decreases in muscle tone), sleep paralysis and hypnagogic
hallucinations, which are intense dream-like imagery before falling asleep
(Dahl, 1992). For a more complete discussion of narcolepsy. The prevalence is
estimated to be 90 in 100 000. Treatment can include a regular schedule of
naps; counseling of family, school and patient; and use of medications,
including stimulants and rapid eye move-ment-suppressant drugs such as
protriptyline. Dahl recommended beginning with standard, short-acting
stimulants, such as MPH, 5 mg b.i.d., and increasing the dose up to 30 mg
b.i.d. if need be.
Selection of a Stimulant Medication as a Treatment Modality
Deciding to Use Medication
The
decision to use stimulant medication in the treatment of ADHD employs different
criteria for each developmental stage. The criteria for use of stimulants in
school-age children and adolescents are well described in the DSM-IV-TR. More
difficulty arises when deciding whether to use these medications in preschool
children, adult patients, patients with mental retardation, or children with
ADHD and comorbid disorders.
Use of Psychostimulants in Children Younger than 6 Years
Unfortunately,
there are only a handful of published treatment studies on preschoolers. No
dose-ranging pharmacokinetic stud-ies have been done in this age group to
determine if younger chil-dren, with their larger liver-to-body size ratio,
might show more accelerated metabolism of psychostimulants than seen in older
children. Therefore, the optimal doses for this age group are not known. To
date there are no studies that would validate or refute clinicians’ concerns
that preschoolers suffer more pronounced stimulant withdrawal effects.
Adults
The
prevalence of ADHD in adults, its severity and indications for treatment are
issues that are not known. Although it had been assumed that children with ADHD
outgrow their problems, prospective follow-up studies have shown that ADHD
signs and symptoms continue into adult life for as many as 60% of children with
ADHD (American Psychiatric Association, 1980). However, only a small percent of
adults impaired by residual ADHD symptoms actually meet the full DSM-IV
childhood criteria for ADHD (Hill and Schoener, 1996). Adults with
concentration problems, impulsivity, poor anger control, job instability and
marital difficulties sometimes seek help for problems they believe to be the
manifestation of ADHD in adult life. Parents may decide that they themselves are
impaired by the same attentional and impulse control problems found during an
evaluation of their ADHD children.
A variety
of medications have been used to treat adults with ADHD. Physicians should be
cautious in the use of these agents until proof of efficacy is available. Of
particular concern is the danger of using psychostimulants in adults with
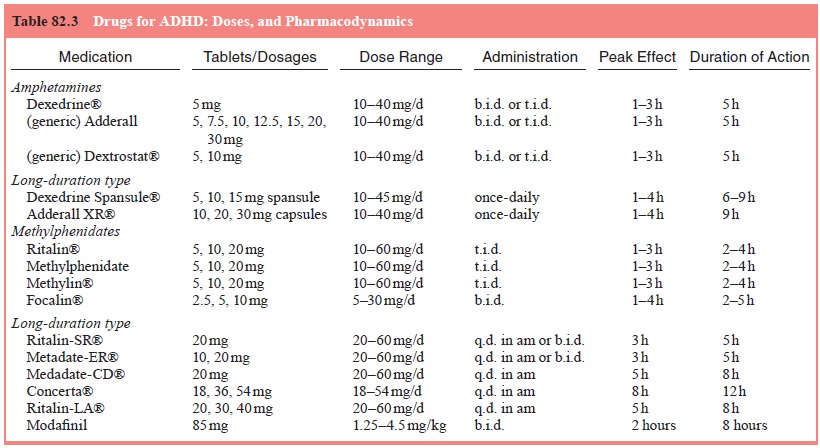
comorbid substance abuse disorder. It would be wise to use MPH because of its
relatively low abuse potential, and because it has been shown in controlled studies
to significantly reduce the symptoms of ADHD in adults (see Table 82.3.)
Continuing Stimulant Treatment in Patients with Tic Disorders
Standard
package instructions for using MPH warns against its use in patients with tics
or in patients with a family history of tics. Patients with Tourette’s syndrome
often have comorbid ADHD. If the two conditions co-occur, concern arises that
stimulant treat-ment – because of its dopamine agonist actions – might unmask,
trigger, accelerate, or precipitate more severe tics.
Tics are
unacceptably worsened for a minority of comorbid children, although reversibly,
and the majority of such comorbid children can be treated cautiously with
low-to-moderate doses of stimulants, particularly MPH (Comings and Comings,
1987).
Patients with Mental Retardation
Many
stimulant treatment studies for school-age children with ADHD exclude children
with full-scale IQs below 70, who are considered to have mental retardation
(MR). This is unfortunate, for the signs of ADHD are far more prevalent in
children with IQs in the MR range (Aman et
al., 1991). Pharmacotherapy reviews involving patients with MR have
reported that institutionalized subjects with severe or profound MR respond
poorly to stimulants. However, studies involving community samples of children
with MR, have shown that these children do respond to MPH. It appears that
children with ADHD who have mild or moderate MR may be more vulnerable to
certain stimulant-related adverse side effects.
Does Comorbidity Affect the Indications for the Use of Stimulant Medication?
ADHD
children that are referred from other physicians may have other Axis I
psychiatric disorders. Extensive literature reviews report that ADHD co-occurs
with conduct and oppositional defi-ant disorder in 30 to 50% of cases, with
mood disorders in 15 to 75% of cases, with anxiety disorders in 25% of cases
and with learning disabilities in 15 to 30% of cases. Clinicians should be
aware that co-morbid ADHD/anxiety disorders may result in lesser response to
treatment more side effects.
Related Topics