Chapter: Maternal and Child Health Nursing : Fetal Development, Placenta Development and Fetal Circulation
Fetal Circulation
Fetal Circulation
The fetus
derives its supply of oxygen and nutrients from the placenta so because of this
the whole of fetal blood has to pass through the organ. The lungs and the
alimentary tract being functionless during pregnancy require only a small blood
supply first to nourish them. The fetus therefore has a blood circulation which
differ from that of its post-natal life, at birth there is a dramatic
alternation in the situation, an almost instantaneous change occurs. All organs
must be mature and normal to take over. The fetal haemoglobin carries 20-30%
more oxygen than adult haemoglobin. This is obtained indirectly from the
maternal circulatory system. Through the umbilical vain that extends from the
placenta oxygen from the chorionic villi enters the placenta through the
umbilical vein and carbondioxide is removed by the umbilical arteries. The
fetus relies on three shunt-like structures to supply Oxygen and nutrient and
to exchange of waste products they are known as temporary structures.
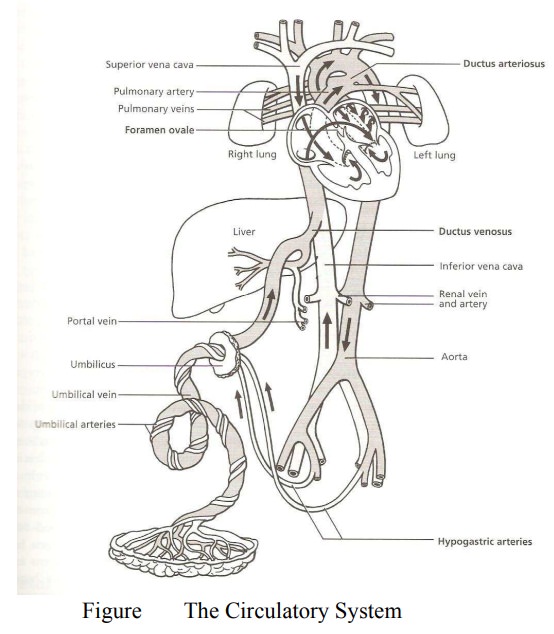
The Temporary Structure
1.
The Ductus venosus: (Vein to vein)This vessel
(pure) carries oxygenated blood that has been form replaced by the placenta the
umbilical vein to the inferior vena cava. It branches just before it reaches
the vena cava to supply the liver.
2.
The Foramen Ovale; (Oval opening) A temporary
opening between the two atria. It allows majority of the blood entering from
the inferior vena cava to pass across from the right atrium to the left atrium.
3.
The Ductus Arteriosus: (Arteries to arteries):
Carries deoxygenated blood from the pulmonary artery to the descending arch of
the aorta enters it just after the subclavia and carotid arteries branch off.
By this it bypasses the pulmonary circulation.
4.
Hypogastric Arteries: These vessels branch off from
the internal ilia arteries and become the umbilical arteries when they enter
the umbilical cord.
5.
The umbilical vein: Carries oxygenated blood from
the placenta to the undersurface of the liver. A branch from it supplies the
liver.
The course of circulation
From the
placenta, the umbilical vein carrying pure oxygenated blood passes through the
abdominal wall to the undersurface of the liver (this is the only vein that
carries pure blood). Just before it joins the Ductus venosus, part of it
branches to supply the liver. The Ductus venosus carries the rest of the blood
to the inferior vena cava where it mixes with the impure blood from the lower
part of the body. The hepatic vein also empties its content into the inferior
vena cava. The blood then enters the right atrium. Most of it (75%) shunt
through the foramen ovale to enter the left atrium and passes into the left ventricle
where it enters the aorta. (it has highest oxygen content in fetal circulation)
and the major portion of it goes via the branches of the arch of the aorta to
–the great vessels of the neck (Coronnal and carotid arteries) to supply the
brain and the heart and the upper limbs also benefit (subclavia arteries). This
ensure that the brain and the heart receive freshly oxygenate blood. The
remaining pass into the descenting arch of the aorta.
The
de-oxygenated blood from the head neck and arms retune through the superior
vena cava to the right atrium, there it joins the small stream from the
inferior vena cava (though not completely mixed) and flow into the right
ventricle. From here the blood passes into the pulmonary artery, small amount
goes to supply the lungs to nourish them while the rest flows through the
Ductus Arteriosus into the aorta. Some are distributed to the abdomen, pelvis,
visceral and the lower limbs, while the rest pass through the hypogastric
arteries which are branches of the internal iliac arteries, into the umbilical
arteries, thus transporting the deoxygenated blood back to the placenta where
interchange between the fetal and the maternal blood takes place for
oxygenation through the processes of osmosis and diffusion and selective action
of cytotrophoblast and syncytiotrophoblast. The impure blood from the legs
return back into the inferior vena cava to join the circulation again the whole
process takes about 30 seconds.
Changes in fetal circulation at birth
The first
important change is brought about by the respiratory effort of the child at
birth. As the baby gasps, takes a breath and cries, the lungs expand and blood
flow into them. The blood which has been passing through the Ductus arteriosus
to the aorta now flows to the lungs.
The
ductus arteriosus which is no more required contracts and closes. It atrophies
to become ligamentum artenosus. The blood now returns from the lungs through
the pulmonary vein to the left atrium.
With the
clamping of the cord circulation in the umbilical vein ceases and the vein
collapses. As a result of this collapse of the umbilical vein, blood no more
flows through the Ductus venosus, it collapses to become the ligamentum
venosus, and later form a support for the portal vein. This result in reduced
pressure of blood in the right atrium, with the establishment of respiration
and enhanced pulmonary circulation the circulation the pressure of blood in the
left atrium increases. These changes of pressure of the two sides of the heart
(Atria) result in closure of the Foramen Ovale, it later become fibrosed and
form the adult inter-atrial septum known as “Fossa valis”.
The
abdominal portion of the umbilical vein gradually atrophies and becomes
fibrosed to form a ligamentum teres which runs between the umbilicus and the
liver, enclosed in a fold of peritoneum known as the falciform ligament.
The
hypogastric and umbilical arteries contract become closed to prevent blood from
escaping. The hypogastric arteries atrophy to become the obliterated
hypogastric arteries except a few centimeters which remain patent and become
the internal iliac and superior vesical arteries.
Conclusion
The ovum
is receptive to fertilization 24 – 48 hour s after ovulation. It is important
to note that the process of fertilization include the journey through the
fallopian tube to the uterus and critically depends on proper preparation of
the reproductive organs systems across the cycle. Successful implantation
depends on the action of progesterone on the cells of the uterine muscle fibers.
The first few weeks of conception happens to be the period when the fetus is
highly vulnerable to congenital abnormalities and factors that can predispose
to this must be avoided. The survivals of the fetus depends on the integrity of
the placenta , so it must be preserved in situ throughout pregnancy , during
pregnancy women must be nutritionally adequate to be able to meet the needs of
the growing fetus
Related Topics