Chapter: Clinical Cases in Anesthesia : Cardiomyopathy Managed With A Left Ventricular Assist Device
Explain the treatment options for dilated cardiomyopathies
Explain
the treatment options for dilated cardiomyopathies.
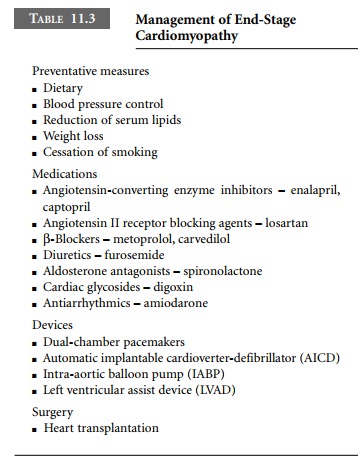
The treatment of DCM is essentially the
symptomatic management of left-sided heart failure (Table 11.3). Four stages of
heart failure are described: initial cardiac injury; neurohormonal activation
and cardiac remodeling; fluid retention and peripheral vasoconstriction; and
ultimate contractile failure. Mild to moderate heart failure is treated with
preventative measures (dietary manipulations, blood pressure control, lowering
of serum lipids, weight loss, and cessation of smoking) in combination with
progressive pharmacologic interventions. Medications are aimed at antagonizing
specific neurohormonal mechanisms of injury and controlling fluid retention.
Beneficial classes of drugs include angiotensin-converting enzyme inhibitors
(e.g., enalapril, captopril), angiotensin II receptor blocking agents (e.g.,
losartan), β-blockers (e.g., carvedilol, metoprolol), diuretics (e.g.,
furosemide), aldosterone antagonists (spironolactone), and digoxin.
Diastolic dysfunction tends to develop as
myocardial function deteriorates, resulting in chronically elevated LA
pressures and, often, atrial fibrillation. In the patient with severe DCM, the
maintenance of sinus rhythm becomes a key factor in maintaining forward cardiac
output, so this population is often placed on antiarrhythmic agents, commonly
amiodarone. When pharmacologic interven-tions fail to maintain sinus rhythm,
dual-chamber (atrio-ventricular sequential) pacemakers are often implanted, for
maintenance of the atrial contribution to diastolic ventricular filling.
Ventricular dysrhythmias cause severe decompensation
and are potentially fatal. To prevent this, an automatic implantable
cardioverter-defibrillator (AICD) is often implanted. As ventricular failure
progresses, symptoms become refractory to outpatient medical therapy. Patients
may require hospitalization for careful fluid management and administration of
positive inotropic, as well as vaso-active agents. At this point, cardiac
transplantation is frequently considered. In the interim, maintenance of
adequate tissue perfusion may require temporary support with an intra-aortic
balloon pump (IABP) or implantation of a left ventricular assist device (LVAD).
The use of implantable LVADs has become common management for intractable
cardiac failure in patients with end-stage cardiomyopathy who are awaiting transplantation.
A number of experimental surgical procedures
(LV reconstruction, dynamic cardiomyoplasty, and others) have been developed to
treat end-stage cardiomyopathy, but results to date have been variable. A
comprehensive review of surgical treatments for heart failure was recently
published by Kumpati et al. (2001).
Related Topics