Chapter: Basic Radiology : Musculoskeletal Imaging
Exercise: Trauma
EXERCISE 6-1.
TRAUMA
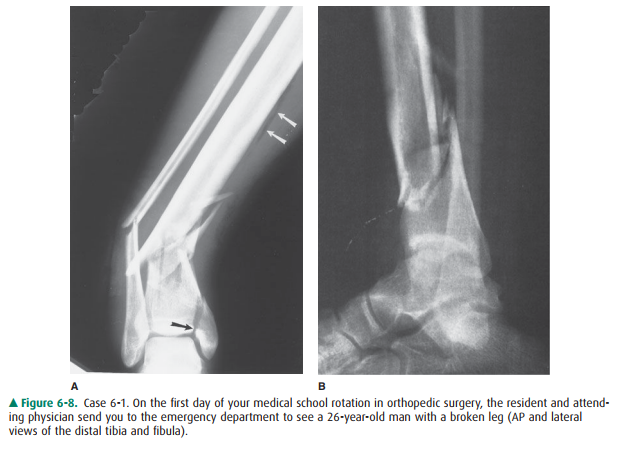
6-1. You are supposed to look at the radiographs for Case 6-1 (Figure 6-8) and call your colleagues in theoperating
room to describe the fracture.
Which of the following statements concerning the fracture would you wish to
make?
A.
The distal tibial fragment is displaced 1 cm ante-riorly.
B.
There is no comminution of the tibial fracture.
C.
There is slight valgus angulation of the distal tib-ial fragment.
D.
This is an open or compound fracture.
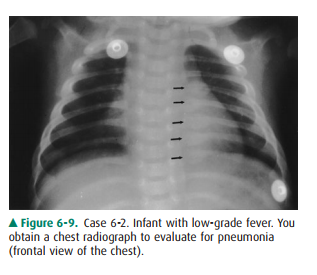
6-2. You interpret
the chest radiograph
for Case 6-2 (Figure 6-9) and render the
following opinion:
A.
Normal chest radiograph
B.
Round pneumonia
C.
Healing rib fractures
D.
Pneumothorax
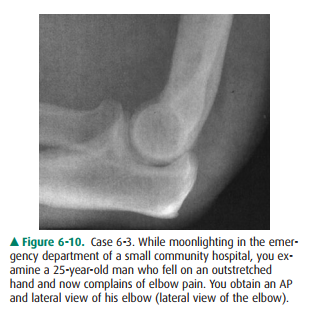
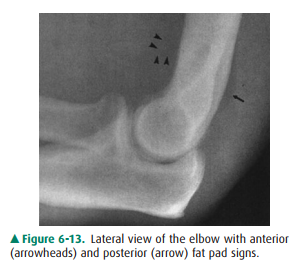
6-3. You first examine
the lateral view of the elbow in Case6-3 (Figure 6-10). You find
A.
a lytic lesion in the distal humerus.
B.
displacement of the fat pads of the elbow.
C.
a fracture through the proximal ulna.
D.
dislocation of the elbow.
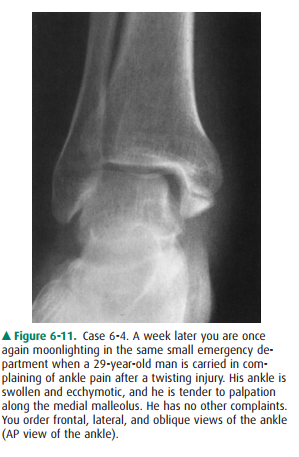
6-4. You examine the
radiographs for Case 6-4. Only the AP view is shown here (Figure 6-11). You
tell the pa-tient he has broken his ankle, but you want to get one more study:
A.
Entire tibia and fibula, to exclude more proximal fractures
B.
Ipsilateral foot, to exclude a fracture of the fifth metatarsal
C.
Contralateral ankle, for comparison purposes
D.
CT, for precise evaluation of the alignment of the fracture
6-5. What is the abnormality in Case
6-5 (Figure 6-12)? should not normally be visible at all. There is no visi ble
fracture or dislocation. (B is the correct answer to Question 6-3).
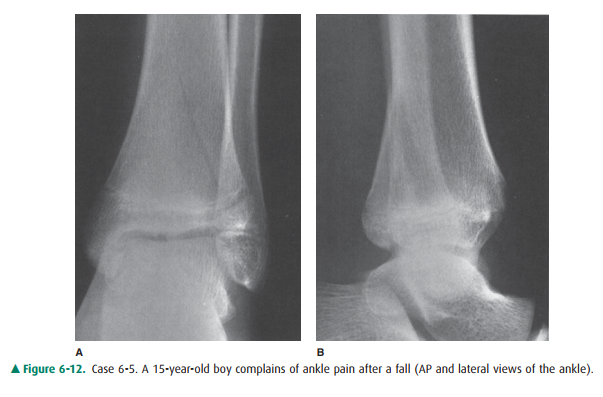
A.Sprain of the lateral ligaments
B.Fracture of the distal fibula
C.Stress fracture of the talus
D.Triplane fracture of the distal tibia
Radiologic Findings
6-1. Figure 6-8 shows
comminuted fractures of the distal tibia and fibula with intra-articular
extension of the tibial fracture (black arrow). The main distal fracture fragment
is displaced posteriorly. As seen on the frontal view, the distal fragments are
angulated so they are pointing medially. Gas density (white ar-rows) indicates
that air has penetrated into the soft tissues through a skin wound, so this is
an open fracture. A fracture line extends to the tibial articu-lar surface
(black arrow) (D is the correct answer to Question 6-1).
6-2. In Figure 6-9, a
row of rounded opacities (arrows) in the left chest represents posterior
healing rib frac-tures (C is the correct answer to Question 6-2).
6-3. This patient‘s
anterior fat pad is pushed away from the bone, creating a small triangular
“sail” (Figure 6-13, arrowheads). The posterior fat pad (arrow) is visible as a
dark line behind the distal humerus, when itaspect of the ankle joint. This
type of fracture is often associated with a more proximal fibular fracture (A
is the correct answer to Question 6-4).
6-5. Abnormal lucencies
run vertically through the epiph-ysis on the frontal view (Figure 6-12) and
obliquely through the metaphysis on both the frontal and the lateral views. The
lateral aspect of the distal tibial ph-ysis or growth plate is widened (D is
the correct an-swer to Question 6-5).
Discussion
Case 6-1: Your mission is to
describe accurately and suc-cinctly the features of this fracture that will
affect treatment and outcome. You should discuss the alignment of the largest
tibial and fibular fragments. Address both displacement and angulation.
Displacement is always described in terms of the position of the distal
fragment relative to that of the proximal fragment. The lateral view shows that
the distal tibial frag-ment is displaced 1 cm posteriorly.
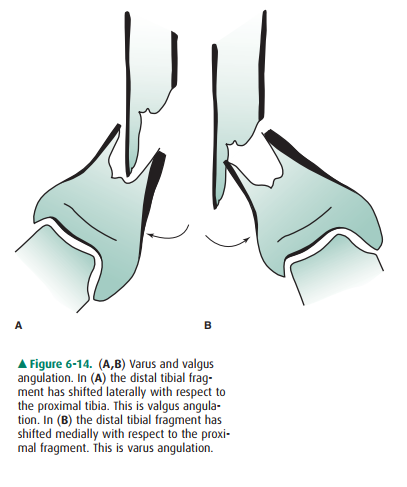
On the frontal view there is
obvious angulation (Figure 6-8 A). Angulation may be described either in terms
of the direction of shift of the distal fragment or in terms of the di-rection
in which the apex of the angle points. In either case, it is better to give a
measurement than to use subjective modi-fiers such as “slight” or “moderate.”
This angulation may cor-rectly be described as “30 degrees of varus angulation
of thedistal fragment” or “30 degrees lateral apical angulation” (Figure 6-14).
Case 6-2: Rib fractures in a
young child suggest child abuse. As most rib fractures in infants are caused by
nonacci-dental injury, you should reexamine the child for other stig-mata of
child abuse, such as bruises, welts, burns, or retinal hemorrhages, notify
protective services, and obtain a skeletal survey. If you are unsure of your
diagnosis or desire confir-mation of the radiographic findings, you should
obtain a ra-diology consult, as discharging the patient could place the child
in serious danger. Figure 6-15 from the skeletal survey reveals the classic
metaphyseal “corner” (large arrows) and “bucket handle”(small arrows) fractures
virtually pathogno-monic of infant abuse. The astute observer will also note a
healing fracture of the superior pubic ramus. In summary, ra-diologic findings
with moderate to high specificity for infant abuse include posterior rib
fractures, metaphyseal fractures, multiple fractures, and fractures at
different stages of healing.

Case 6-3: When examining a
radiograph for a suspected fracture, it is important to evaluate not only the
bones themselves but also the adjacent soft tissues. In a number of areas of
the body there are normal deposits of fat, termed fat pads, which may be
displaced by accumulation of blood or fluid in the underlying tissues. The fat
pads of the elbow are particularly helpful. Displacement of the elbow fat pad
is a nonspecific sign that indicates distension of the joint. Effusions due to
rheumatoid arthritis, an infected joint, orhemorrhage, especially in a patient
with bleeding disorder, could all cause the “fat pad sign” seen in this
patient. In an otherwise healthy person who has suffered trauma, however, a
radial head fracture should be suspected because it is the most common elbow
fracture in an adult. This patient’s frontal view did actually demonstrate a
small lucent frac-ture line in the radial head. Even without that, however, the
most prudent course is to treat the patient as though he had a radial head
fracture with immobilization and arrange for follow-up care with a physician
accustomed to caring for fractures.
Case 6-4: Transverse medial
malleolar fracture usually ac-companies eversion of the ankle and is often
associated with a fibular fracture. The fibular injury may occur at any level
from the ankle to the knee. When there is no apparent distal fibular fracture
on ankle views, the remainder of the bone should be imaged. In this case, there
is, indeed, a fracture ofthe proximal fibula (Figure 6-16). This fracture is
also called the “Maisonneure” fracture, named for the surgeon Jules Germain
Francois Maisonneure, and indicates rupture of the interosseous membrane all
along its course from the ankle to the fibular fracture. This is an unstable
injury that many orthopedic surgeons will treat with open reduction and
in-ternal fixation of the malleolar component and of the syndesmosis. Fractures
of the proximal fifth metatarsal may accompany ankle inversion and may be
difficult to distin-guish clinically from other ankle injuries. Therefore, this
part of the foot should always be included on at least one view of the ankle.
If it is not, then it is prudent when possible to obtain one more view, but
this should not ordinarily be considered a separate study or incur an
additional charge. CT is not neces-sary in this situation.

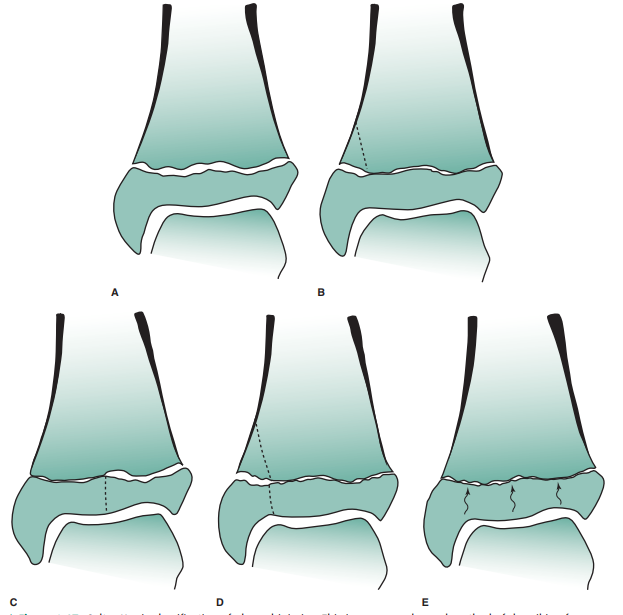
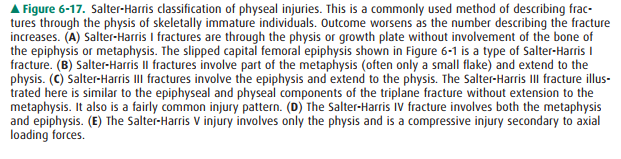
Case 6-5: This adolescent patient
has suffered a relatively common growth plate injury with a typical but
somewhat complex fracture pattern. It is called a “triplane” fracture be-cause
it has components that run, more or less, in all three primary planes of
section. It travels in the sagittal plane through the epiphysis, in the axial
plane through the un-fused portion of the physis or growth plate, and in the
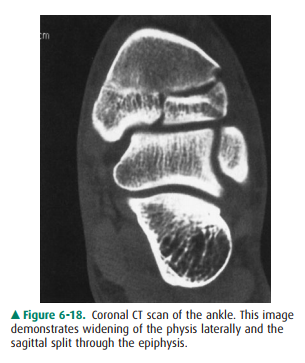
coronal plane through the metaphysis. It is a Salter-Harris type IV fracture (Figure
6-17). It can be diagnosed on the conventional radiographs. Overlapping of
several bones in the ankle region, together with the inferiorly concave shape
of the articular surface of the distal tibia, the tibial plafond, complicates
evaluation of fracture fragment position, and so a CT scan was obtained (Figure
6-18).
Related Topics