Chapter: Forensic Medicine: Post-mortem changes
Early post-mortem changes
Early post-mortem changes
Post-mortem cooling (algor mortis)
Energy, therefore heat, is produced in the body
by metabolic processes. The temperature control mechanism in the brain is
responsible for maintaining normal oral temperature at between 36 and 37,28 C,
regardless of fluctuation in the outside temperature. Rectal temperature is
about 0,3 to 0,48 C higher. Heat is spread through the whole body by the circulation
and is then lost during different processes:
·
radiation or emission
·
conduction from the body to other substances or materials in contact
with it - this
is not important in the living person, but becomes important post mortem (eg
heat transmitted and lost when a body is lying on a cold cement floor)
·
convection or the process by which the air in immediate contact with a
warmer body is heated and expands in volume, becomes lighter (less dense),
rises and is replaced by colder and denser air
·
evaporation, mostly by perspiration
When the person dies and the circulation ceases,
this internal spread or diffusion of heat no longer takes place. The body
surface cools off while the deep or so-called core temperature is still
maintained for some time. At death certain metabolic processes still continue
for some time, especially in the liver and the muscles, thus producing heat.
The core temperature (which is usually taken in the rectum or just beneath the
liver) will thus not fall immediately, but remain constant while the surface
temperature already starts dropping. The drop in the core temperature will
therefore start later when a gradient between core and surface has been
established.
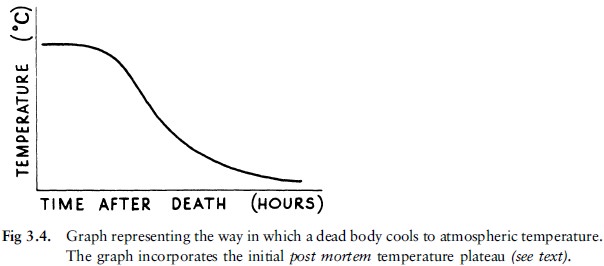
When these temperature changes are represented
graphically there is an initial delay phase due to metabolic processes which
still continue for some time, and the fact that a gradient must first be
established between the internal (core) and external (surface temperature) of
the body. The decrease in temperature (which follows the initial delay phase)
does not occur linearly: initially the gradient between the outside and body
temperature is big, and the heat loss is rapid, but as this difference/gradient
decreases, the temperature decrease is also slower. This temperature curve is
presented graphically in figure 3.4.
In the assessments it is therefore important
that the core temperature is measured and applied.
Except in cases where the external temperature
is at freezing point, the body temperature seldom reaches the external
temperature, due to the production of heat by bacteria involved in the
decomposition process.
There are a number of formulae or normograms of
body temperature that can be used to determine the moment of death, but they
should not be applied conclusively; only as guidelines.
Factors that influence post-mortem cooling
a Initial body temperature
Certain conditions during life such as
infections, reactions to medications, etcetera, can cause fever and thus a rise
in body temperature. Hypothermia (subnormal body temperature) will have the
opposite effect. According to the formulae used, body temperature at the moment
of death is regarded as 36,9 8C.
b External temperature
The external temperature determines the gradient
and therefore the rate of cooling. If the external temperature is higher than
37 8C, obviously no cooling will take place.
c Physical characteristics
Fat provides good insulation against heat loss.
An obese person therefore loses heat more slowly than a lean person. Babies
also have a large body surface relative to their weight, and cool off more
rapidly. Especially the surface of a baby's head is disproportionately large
compared to the rest of the body. Oedema and dehydration also have an effect;
heat loss is more rapid in a dehydrated person.
d Body posture
Any position which minimises the area of the
body surface exposed to air or a cold surface will slow down the cooling
process. A body curled up in the foetal position will therefore cool off more
slowly than a stretched-out body, all the other factors being the same.
e Air movement and humidity
Air in motion can precipitate cooling, as it
accelerates convection and conduction. This is also called the wind factor.
Humid air promotes heat loss.
f Clothing and other coverings
Clothes slow down heat loss by conduction and
convection. Wet clothes speed up heat loss.
g Medium in which body lies
A body lying in water loses body heat more rapidly
than one outside due to greater heat loss as a result of increased convection
and conduction in water as opposed to air. The type of water (fresh water or
sea water) plays no role; only the temperature of the water. Sewage water may
have a higher temperature due to heat produced by micro-organisms.
Post-mortem muscle changes
The muscles of the body go through three phases
after death.
·
Primary muscle flaccidity occurs immediately at death, as a result of
loss of muscle tone. The body becomes limp. An exception, the so-called
cataleptic stiffness (rigor) is discussed elsewhere.
·
Rigor mortis or post-mortem stiffness then follows (fig 36A
and B as well as photo 1).
·
Secondary muscle flaccidity commences at the onset of the putrefaction
process when the muscles start to relax finally and permanently.

Rigor mortis
Rigor mortis occurs as a result of
physio-chemical reactions in all the muscles of the body due to a decrease in
adenosine triphosphate (ATP). ATP is required for both muscle contraction and
relaxation. At death the muscles continue consuming ATP. Simultaneously lactate
(milk acid) is produced by anaerobic (oxygen-independent) respiration. The
decreased ATP levels as well as the changed pH levels result in rigor mortis.
Rigor mortis usually sets in 3 to 6 hours after
death. It is first observed in the smaller muscles which, inter alia, are
connected to smaller joints such as in the hands and face, and can therefore
easily be immobilised. The arms and thorax follow and eventually the large
muscles of the feet and legs. Rigor mortis usually spreads throughout the body
after 10 to 12 hours and disappears after approximately 36 hours. It is
generally accepted that rigor mortis disappears in the same sequence in which
it has set in, namely first the groups of smaller muscles, followed by the
groups of muscles gradually increasing in size.
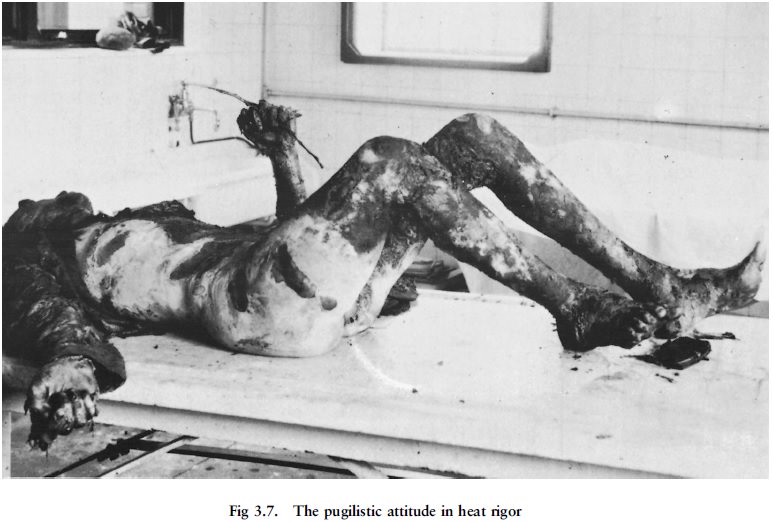
Rigor mortis is not associated with shortening
(contraction) of the muscles. Therefore the limb joints do not bend or flex
under the influence of rigor mortis. Please note that the so-called boxer's or
pugilistic attitude in burnt bodies is the result of shortening of the muscles
when the proteins or albumin coagulate and denaturate as a result of the heat.
In individuals with low muscle mass, like babies
and emaciated persons, hardly any or no rigor mortis may develop.
Rigor mortis is not necessarily an indication of
the posture/position of the body at the moment of death. It merely represents
the position in which the body was at the time of the development of rigor
mortis. Paradoxal rigor mortis is observed, for example, when a leg sticks out
over a bed without being in contact with the floor; the body was thus
apparently moved after rigor mortis had developed, otherwise the leg would have
bent at the knee under the effect of gravity and would have become fixed in
that position.
If rigor mortis is broken, it will not set in
again. This occurs mostly during handling of the corpse, for example when the clothes
are removed.
Factors which influence the appearance and disappearance of rigor mortis
a Temperature
When the external temperature is high, the onset
of rigor mortis is accelerated and its duration shortened. A low external
temperature inhibits the onset and lengthens the duration. If bodies are
exposed to temperatures below 108 C, it is exceptional for rigor mortis to set
in, but when the body is placed in a warmer environment, it sets in as usual.
(Please see rigidity as a result of cold, below.)
The higher the body temperature, the more rapidly rigor mortis will set in and also disappear. The more rapid heat loss in children, as explained above, is the reason why rigor mortis sets in more rapidly in their bodies.
b Muscle condition at the time of death
Strenuous pre-death exercising decreases the ATP
content of the muscles and thus accelerates the onset as well as subsequent
disappearance of rigor mortis. The same mechanism is relevant in deaths caused
by electrocution or after convulsions as there is increased muscle activity and
thus lower ATP levels at the time of death.
Specific manifestations
a Cataleptic stiffening (cadaveric spasm)
This condition sets in where the muscles which
at the moment of somatic death are in a condition of normal contraction, stay
in that condition during the whole period of cellular death, while the other
muscles are in a state of primary flaccidity. Cataleptic stiffness (rigidity)
will last till rigor mortis has set in in the other muscles, and will then
disappear when rigor mortis disappears. Although it usually affects only one
muscle group, like the hand muscles, it can sometimes affect more or even all
the muscles.
This rare form of rigidity sets in when the
person dies during a very stressful period and somatic death sets in very
rapidly. It appears as if the continued contraction is due to the failure (for
some obscure reason) of the chemical processes required for active muscle
relaxation during cellular death.
In cataleptic stiffening there is thus no
relaxation phase of the muscles. This type of stiffening has been seen in
mountain climbers who fell to their death and in a last fruitless attempt
grabbed at a branch; after death the branch was firmly grasped in the hand. The
same applies to a small percentage of suicide cases, where the firearm was
grasped in the hand. More extreme cases of cataleptic rigor have been noted in
soldiers dying during a military charge.
Cataleptic spasm can be imitated after death if
an object is placed in the hand in such a way that the onset of rigor mortis
will clench it in a grip: The difference is that in cataleptic spasm only the
hand that grips the object has stiffened; the other muscles are limp.
b Rigidity due to heat
When a body is exposed to heat, the proteins
denaturate and coagulate (break up and solidify) in the muscles, and the
muscles shorten. As the flexor muscles are bigger and stronger than the
extensor (stretch) muscles, they dominate the smaller muscles, and the body
takes on the typical posture of a boxer (fig 3.7). The shortening can be such
that the muscles tear, also causing laceration wounds of the overlying skin and
soft tissue.
Rigor mortis does not develop in muscles that
stiffened due to heat, but the latter can set in after rigor mortis.
Heat stiffening and the concomitant body posture
is therefore a post-mortem phenomenon, and not an indication of the body
posture or position of the limbs at the time of death.
c Rigidity due to cold
Cold rigidity sets in when the body is exposed
to temperatures under 3,5o C. Babies and young children have a thick
subcutaneous layer of fat, and this rigidity is then often prominent because
the fat ``stiffens'' and makes the body less flexible. This is also true of fat
people where cold rigidity is more prominent than in slim persons. When the
body later heats up, true rigor mortis can set in, although the ice crystals
often damage the muscle cells and may prevent rigor mortis.
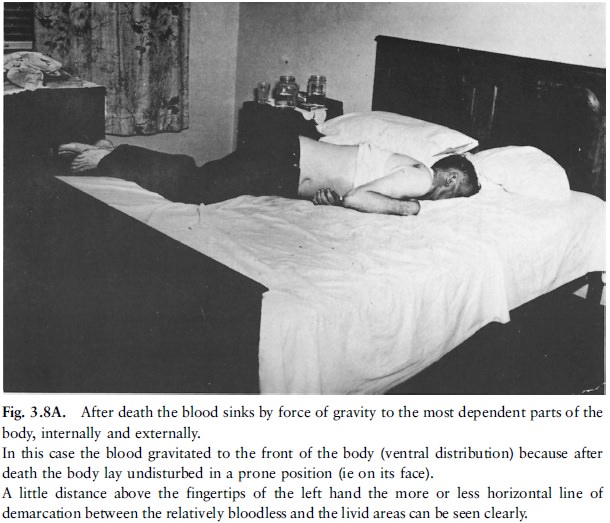
Hypostasis (livores mortis)
There are several synonyms for this condition,
namely lividity, death spots and post-mortem discoloration. About one hour
after death the blood in most bodies becomes permanently fluid because of the
release of fibrinolysin from the endothelial lining of the blood vessels. The
blood cells gravitate to the dependent or lowest parts of the body (fig 3.8A
and B). This gravity-dependent movement of blood discolours the skin as well as
internal organs to a reddish-blue colour. In a body in the hanging position the
hypostasis will therefore appear in the hands/forearms and feet/lower legs.
The fluid component of blood (plasma) also
gravitates to a lesser extent and causes oedema and later even skin blistering.
Sometimes the capillary veins can also rupture, and then petechial haemorrhages
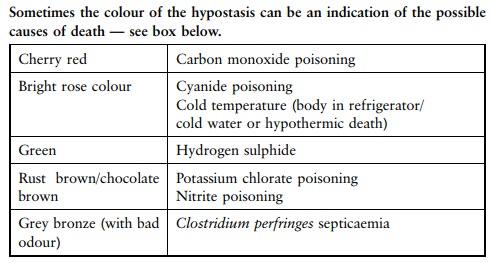
set in, which can converge and even form blood blisters. The colour of the
complexion determines how readily hypostasis will be visible on the skin.
In a person who was exsanguinated (``bled out'') before death, this condition is often less obvious because of the fact that very little blood remained in the circulation.
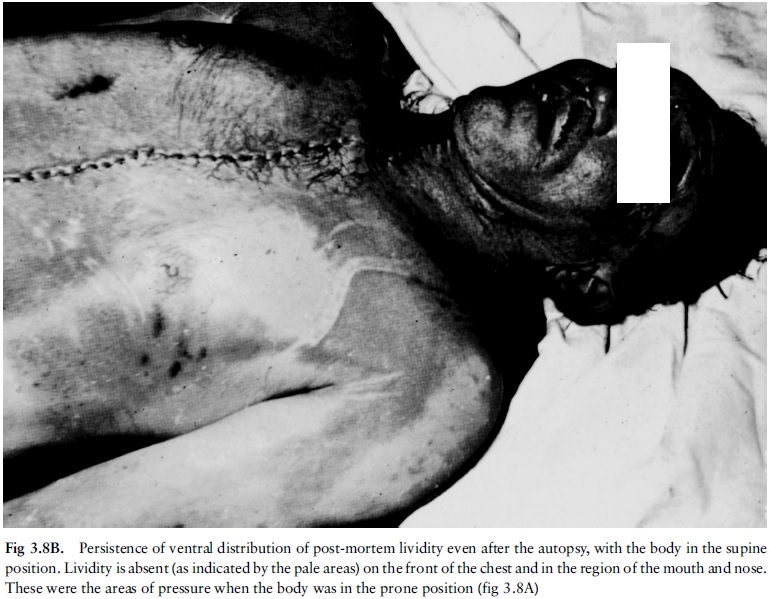
Hypostasis does not develop in areas where
pressure is exerted on the body, in other words where the capillary veins are
compressed by pressure. In the supine position the body will have no hypostatic
changes over the buttocks, shoulders and the parts in contact with the surface
on which it lies. It will not develop where a garment or buckle is tightly pressed
against the body. Thus there will often be an area of peri-oral pallor around
the mouth when the body lies prone with the head downwards, for instance on a
pillow; it must not be confused with the application of force as in suffocation
where pressure on the mouth is applied.
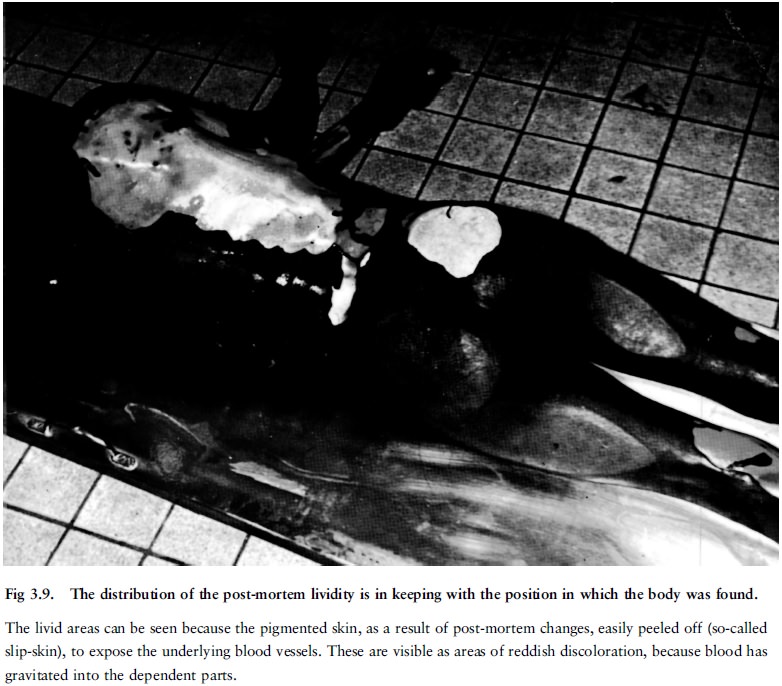
Hypostasis thus does not necessarily give an
indication of the position in which the person has died, but only an indication
of the position of the body when the hypostasis set in. In can be of assistance
to confirm whether the corpse was moved after death when the hypostasis is
contradictory to the position in which the body was found (eg hypostasis over
the back, but the body was found in a prone position).
The time that it takes for hypostasis to develop
varies. Sometimes it is already visible before death, for example in a person
who is terminally in a state of cardiac failure with a slow blood circulation.
Usually it is maximally developed 12 hours after death.
Initially hypostasis can shift to other parts of the body, if the body is moved after hypostasis had already developed. However, after the red blood cells started haemolysing the haemoglobin (blood colourant) will leak out in the vessel walls as well as surrounding tissue and discolour it to a reddish purple hue. Then the hypostasis will not shift any more, even if the body is moved. The hypostasis is then fixed. However, hypostasis will then also develop in the ``new'' dependent areas.
Conditions that have to be distinguished from hypostasis
Bruises
The location and shape of a discoloration can
distinguish it from hypostasis, but the indisputable evidence is only to be
found when the skin is incised. In the case of a bruise the blood is
extravasated (ie discharged from a vessel) or diffused into the tissue; in the
case of hypostasis it is still limited to the vessels. Microscopy can be of
further assistance if the naked eye cannot detect the difference.
Inflammatory changes
Inflammation causes increased blood circulation
in the affected tissue and it can, for example, imitate hypostasis in a lung,
where there was in fact pneumonia, or in the heart, where there was in fact a
myocardial infarction. Microscopy is again necessary to find the final answer.
Related Topics