Chapter: Essentials of Psychiatry: Dissociative Disorders
Dissociative Disorders
Dissociative Disorders
Dissociative phenomena are best understood through the term désagrégation (disaggregation)
originally given by Janet (1920). Events
normally experienced as connected to one another on a smooth continuum are
isolated from the other mental processes with which they would ordinarily be
associated. The dissocia-tive disorders are a disturbance in the organization
of identity, memory, perception, or consciousness. When memories are sep-arated
from access to consciousness, the disorder is dissociative amnesia.
Fragmentation of identity results in dissociative fugue or dissociative
identity disorder (DID; formerly multiple per-sonality disorder). Disintegrated
perception is characteristic of depersonalization disorder. Dissociation of
aspects of conscious-ness produces acute stress disorder and various
dissociative trance and possession states. Numbing and amnesia are diagnos-tic
components of post traumatic stress disorder (PTSD). These dissociative and
related disorders are more a disturbance in the organization or structure of
mental contents than in the contents themselves. Memories in dissociative
amnesia are not so much distorted or bizarre as they are segregated from one
another. The identities lost in dissociative fugue or fragmented in DID are two-dimensional
aspects of an overall personality structure. In this sense, patients with DID
suffer not from having more than one personality but rather from having less
than one personality. The problem involves information processing: the failure
of inte-gration of elements rather than the contents of the fragments.
The dissociative disorders have a long history in classical
psychopathology, being the foundation on which Freud began his explorations of
the unconscious and Janet developed dissociation theory. Although much
attention in psychiatry has shifted to di-agnosis and treatment of mood,
anxiety and thought disorders, dissociative phenomena are sufficiently
persistent and interesting that they have elicited growing attention from both
professionals and the public. There are at least four reasons for this:
They are fascinating phenomena in and of
themselves, involv-ing the loss of or change in identity, or memory, or a
feeling of detachment from extreme and traumatic physical events.
·
Dissociative disorders seem to arise in response to
traumatic stress.
·
Dissociative disorders remain an area of
psychopathology for which the best treatment is psychotherapy, although
adjunc-tive pharmacological interventions can be helpful.
·
Dissociation as a phenomenon has much to teach us
about information processing in the brain.
Development of the Concept
The
dissociative disorders might have been studied more inten-sively during the
20th century had not Janet’s and Charcot’s workbeen so
thoroughly eclipsed by Freud’s psychoanalytic theory, emphasizing as it did
repression rather than dissociation.
Hilgard (1977) developed a neodissociation theory that re-vived interest
in Janetian psychology and dissociative psychopa-thology. He postulated
divisions in mental structure that were hori-zontal rather than vertical, as
was the case in Freud’s archeological model. This model allowed for immediate
access to consciousness of any of a variety of warded-off memories, which is
not the case in Freud’s system. In the dynamic unconscious model, repressed
memories must first go through a process of transformation as they are accessed
and lifted from the depths of the unconscious, for ex-ample, through the
interpretation of dreams or slips of the tongue. In Hilgard’s model, amnesia is
a crucial mediating mechanism that cre-ates barriers dividing one set of mental
contents from another. Thus, flexible use of amnesia is conceptualized as a key
defensive strategy. Therefore, reversal of amnesia is an important therapeutic
tool.
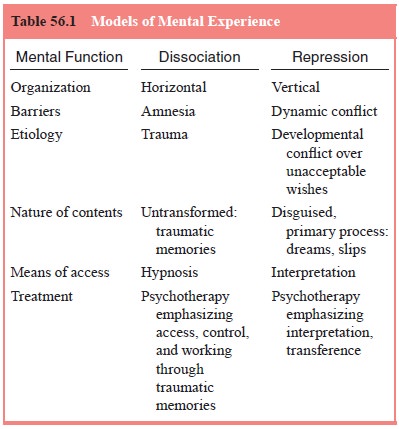
Repression as a general model for keeping information out of conscious
awareness differs from dissociation in four impor-tant ways:
· In repression, information is disguised as well as hidden. Dis-sociated
information is stored in a discrete and untransformed manner, for example, as a
memory of some element of a trau-matic experience, whereas repressed
information is usually disguised and fragmented. Even when repressed
information becomes available to consciousness, its meaning is hidden, for
example, in dreams or slips of the tongue.
· Retrieval of repressed information requires translation. Re-trieval of
dissociated information can often be direct. Tech-niques such as hypnosis can
be used to access warded-off memories. By contrast, uncovering of repressed
information often requires repeated recall trials through intense question-ing,
psychotherapy, or psychoanalysis with subsequent inter-pretation (i.e., of
dreams).
· Repressed information is not discretely organized temporally. The
information kept out of awareness in dissociation is often for a discrete and
sharply delimited time, whereas repressed information may be for a type of
encounter or experience scat-tered across times.
· Repression is less specifically tied to trauma. Dissociation seems to be
elicited as a defense most commonly after epi-sodes of physical trauma, whereas
repression is in response to warded-off fears, wishes and other dynamic
conflicts.
Whether dissociation is a subtype of repression or vice versa, both are
important methods for managing complex and affec-tively charged information.
Given the complexity of human in-formation processing, the synthesis of
perception, cognition and
affect is a major task. Mental function is composed of a variety of
reasonably autonomous subsystems involving a perception, memory storage and
retrieval, intention and action. Indeed, the accomplishment of a sense of
mental unity is an achievement, not a given. It is remarkable not that
dissociative disorders occur at all, but rather that they do not occur more
often. Models of mental experience are presented in Table 56.1.
Related Topics