Chapter: Clinical Cases in Anesthesia : Noncardiac Surgery After Heart Transplantation
Describe the physiology of transplanted hearts
Describe the physiology of transplanted hearts.
The donor heart is denervated during
harvesting. Consequently, the recipient lacks efferent and afferent
innervation. The transplanted heart does not receive auto-nomic or somatic
input. Although denervation prevents responses to extrinsic neural signals,
intrinsic myocardial mechanisms and reflexes remain intact. While transplanted
hearts function in isolation from the nervous system, they respond to humoral
factors (e.g., catecholamines) circulating in blood.
The results of cardiac denervation are:
·
Relative
tachycardia from absent vagal input to the trans-planted heart. Heart rates
approximate 90–100 beats per minute.
·
Loss of
rapid heart rate responses to autonomic reflexes. Heart rates remain unchanged
with carotid mas-sage, acute hyper- or hypotension, and from Valsalva
maneuvers.
·
Absence
of many pharmacologic effects. Drugs which alter the heart rate indirectly, via
the autonomic nervous system, will not have their usual effects on the trans-planted
heart. Vagolytic drugs, such as atropine, pan-curonium, and meperidine, will
not increase heart rate. Vagotonic drugs, such as acetylcholinesterase
inhibitors and opioids, will not decrease heart rate. Medications with both
direct and indirect cardiac actions will maintain their direct effects on the
denervated heart. Digoxin, for example, maintains its positive inotropic
effects on the graft, but will not slow heart rate through its
parasympa-thetically mediated effects on the atrioventricular (AV) node.
·
Delayed
and attenuated responses to laryn-goscopy, intubation, painful stimuli, and
light anesthe-sia because direct sympathetic innervation of the heart no longer
occurs. However, prolonged stimulation results in rising levels of circulating
catecholamines that will eventually induce an increase in heart rate, or even
an exaggerated one, directly through myocardial adrenergic receptors.
·
Inability
to perceive angina. Despite sporadic case reports to the contrary, which have
been touted as evidence of reinnervation, the majority of post-transplantation
patients do not perceive angina.
Despite denervation, intrinsic myocardial
mechanisms remain intact in the transplanted heart:
·
The
denervated myocardium responds normally to circulating or administered
catecholamines (e.g., epi-nephrine, norepinephrine) and direct-acting
sympath-omimetic agents (e.g., isoproterenol, dobutamine) directly through
myocardial adrenergic receptors. In this regard, denervation appears to induce
downregulation of β1 receptors, so most β-adrenergic receptors on the denervated
myocardium will be β2 subtypes.
·
The
Frank-Starling mechanism (increased preload results in increased stroke volume)
remains intact, and is the primary mechanism for increased cardiac output
during exercise or stress. For this reason, it is important to maintain
adequate preload in post-transplantation patients. Since they already have
elevated heart rates, the only way a post-transplant patients can initially
increase cardiac output is through the Frank-Starling mechanism. Any further
increases in heart rate and cardiac output with prolonged exercise or stress
are the result of increased levels of circulating catecholamines, and are therefore
slightly delayed in onset (and in resolution).
· Metabolic autoregulation of coronary blood flow
in response to changes in pH and pCO2 remains intact.
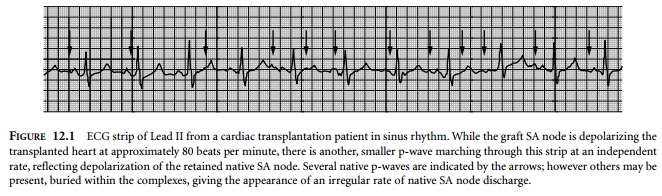
·
Normal
electrical impulse formation and conductivity along the usual pathways is
maintained in the trans-planted heart. Classic orthotopic heart transplantation
techniques leave cuffs of native right and left atrial tissue behind in the
recipient, to facilitate surgical anasto-moses. The native sinoatrial (SA) node
is contained in the right atrial cuff. Impulses continue to emanate from the
native SA node, but these can not cross atrial suture lines and do not
depolarize the transplanted heart. Frequently, two independent p-waves are
dis-cernible on the post-transplant electrocardiogram (ECG) (Fig. 12.1).
Physiology
of the Transplanted Heart
Cardiac denervation
·
Resting
tachycardia of 90–100 beats/min
·
Due to
vagus nerve denervation
·
Absence
of autonomic reflexes
·
No
change in heart rate to:
§ carotid massage
§ Valsalva maneuver
§ atropine
§ pancuronium
§ meperidine
§ acetylcholinesterase inhibitors
§ opioids
§ digoxin
o
Delayed
tachycardic response to:
§ hypotension
§ painful stimuli
§ light anesthesia (mediated through
cate-cholamine release)
o
Phenomenon
of reinnervation remains speculative
·
Intrinsic
myocardial mechanisms
·
Normal
response to:
o
Circulating
catecholamines (epinephrine, norepinephrine)
o
Direct-acting
sympathomimetics (isoproterenol, dobutamine)
·
Frank-Starling
mechanism remains intact:
o
Primary
mechanism to increase cardiac output
o
Important
to maintain adequate preload
·
Metabolic
autoregulation of coronary blood flow:
o
Responds
to local pH and pCO2 Normal electrical impulse formation and
o
conduction:
·
Action
potentials from native SA node do not cross suture line and are not propagated
to donor heart
Related Topics