Chapter: Microbiology and Immunology: Bacteriology: Mycobacterium leprae and Mycobacterium
Clinical Syndromes - Mycobacterium leprae
Clinical Syndromes
◗ Leprosy
M. leprae causes leprosy, a chronic granulomatous disease. Theclinical manifestations of leprosy depend on immune status of the host and spread of the bacilli. It is classified into five groups as: (a) tuberculoid leprosy, ( b) borderline tuberculoid leprosy, (c) mid-borderline leprosy, (d) borderline lepromatous leprosy, and (e) lepromatous leprosy. The incubation period varies from 6 months to 40 years or longer. The mean incubation period for tuberculoid leprosy is 4 years and for lepromatous leprosy is 10 years.
Tuberculoid leprosy: Skin lesions are few. These are usu-ally circular, or serpiginous, sharply demarcated and often hypopigmented. These lesions may have raised and erythem-atous border with a dry scaly appearance in the center with complete anesthesia. The skin lesions are commonly found on the face, limbs, buttocks, or elsewhere but are not found in the axilla, perineum, or scalp.
Neural involvement is common in tuberculoid leprosy. The ulnar, peroneal, and greater auricular nerves are involved, lead-ing to tender, thickened nerves with subsequent loss of func-tion. Damage of the nerve can result in wrist drop or foot drop.
Borderline tuberculoid leprosy: Lesions in this form ofleprosy are similar to those seen in the tuberculoid leprosy, but are smaller and more numerous. Skin lesions are few, asymmet-ric, and with nearly complete anesthesia. Peripheral nerves are thickened and involved asymmetrically. This form of leprosy may remain at this stage or can regress to the tuberculoid form; or it can progress to lepromatous form.
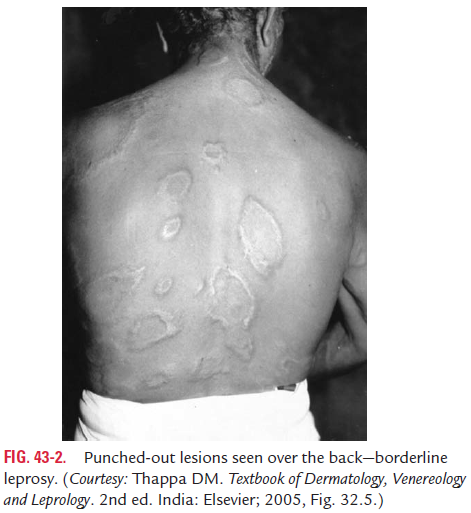
Mid-borderline leprosy: Skin lesions in this type of leprosyconsist of numerous unequally shaped plaques that are less well defined than in the tuberculoid types. These skin lesions are distributed asymmetrically (Fig. 43-2, Color Photo 46). Anesthesia is moderate, and the disease can remain in this stage, can improve, or worsen.
Borderline lepromatous leprosy: Skin lesions are moderateto numerous. They are slightly asymmetrical with slight or no anesthesia. Peripheral nerves are enlarged moderately and sym-metrical. Like the other forms of borderline leprosy, the disease may remain in this stage, improve, or worsen.
Lepromatous leprosy: The skin lesions include macules,nodules, plaques, or papules. The skin lesions are extensive and are bilaterally symmetrical. They are most severe at the cooler parts of the body. This form of disease is associated with dis-figurative lesions. The skin of the face and forehead becomes thickened and corrugated, giving rise to typical leonine face. The lateral part of the eyebrows may be lost. Other disfigur-ing lesions include pendulous ear lobes, hoarseness of voice, involvement of cornea (Color Photo 47), perforation of the nasal septum, and nasal collapse.
Painless inguinal and axillary adenopathy, scarring of testis leading to sterility and gynecomastia are other complications. Diffuse hyperanesthesia involving peripheral parts of extremi-ties also occur due to involvement of the neural tissue.
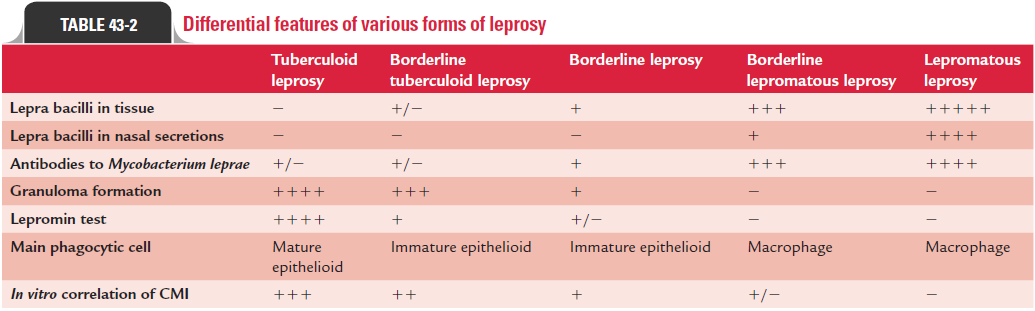
Differential features of various forms of leprosy are summa-rized in Table 43-2.
◗ Lepra reactions
The course of leprosy may be interspersed with reactional stage, which occurs in one-third of the patients. These reactions are of allergic nature and are acute inflammation of the disease and are known as lepra reactions. These reactions are consid-ered a medical emergency, requiring immediate treatment and management. Such leprous reactions include: (a) lepra type I (reversal) reaction, (b) lepra type II reaction or erythema nodo-sum leprosum (ENL), and (c) lucio phenomenon.
Lepra type I reaction: Lepra type I reaction is a type IV cell-mediated allergic hypersensitivity. This reaction is seen mostly in patients with borderline leprosy, occurring spontaneously or more often during chemotherapy. These reversal reactions usually suggest a shift toward tuberculoid form after start of chemotherapy. This type I response is precipitated by puberty, pregnancy, and childbirth. This reaction usually occurs during the first 2 months of therapy to up to 12 months. These reac-tions are characterized by development of skin erythema with edema and tenderness of peripheral nerves.
Lepra type II reaction: Lepra type II reactions are type IIIhumoral hypersensitivity reactions with systemic inflam-matory response due to deposition of immune complexes. This condition occurs in 20% of patients with lepromatous leprosy and in 10% of patients with borderline leprosy. This reaction occurs after a few years of therapy and relapse inter-mittently over several years. Appearance of crops of painful erythematous nodules on the skin and subcutaneous tissue is the characteristic manifestation. Fever, malaise, arthralgia, neuralgia, iridocyclitis, arthritis, and proteinuria are other symptoms.
Lucio phenomenon: Lucio phenomenon is an unusual formof type II reaction. The condition manifests as cutaneous hemorrhagic infarct in patients with diffuse lepromatous lep-rosy. This condition is commonly documented in Mexico and Central America.
Related Topics