Chapter: Medical Microbiology: An Introduction to Infectious Diseases: Chlamydia
Chlamydia trachomatis Diseases
Chlamydia trachomatis DISEASES
Ocular trachoma, with progressive inflammation and scarring leading to blindness, has been recognized since antiquity, but the role of Chlamydiae in conjunctivitis and pneumonia in young infants, and in a variety of genital infections was only clarified during the past 40 years. Like trachoma, the genital infections can persist or recur, with chronic sequelae.
EPIDEMIOLOGY
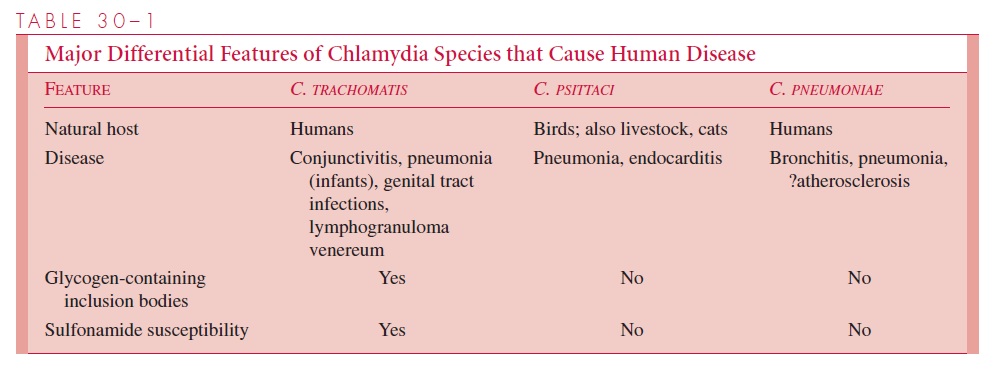
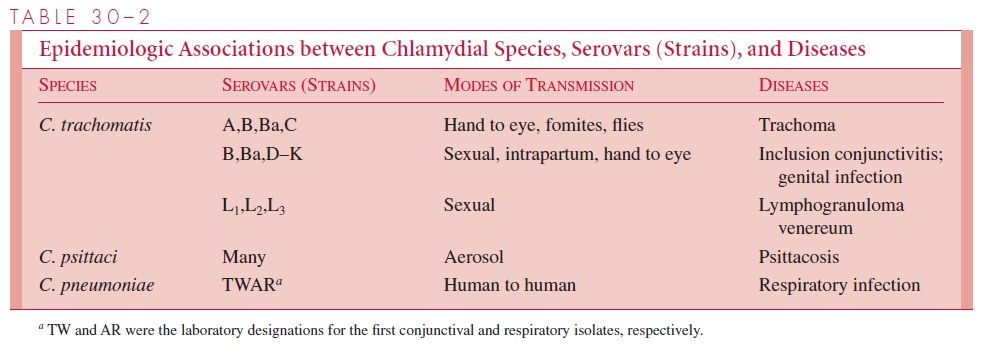
C. trachomatis causes disease in several sites, including the conjunctiva and genital tract.It is spread by secretions and is the most common sexually transmitted disease. In the United States over 700,000 cases are reported each year, which is twice the number for gonorrhea. Humans are the sole reservoir (see Table 30 – 1). Each of the major disease syndromes caused by chlamydiae are associated with several different strains (see Table 30 – 2). Inclusion conjunctivitis is seen among population groups in which the strains causing C. trachomatis genital infections are common. This disease is the most common form of neonatal conjunctivitis in the United States, occurring in 2 to 6% of newborn in-fants. The infection results from direct contact with infective cervical secretions of the mother at delivery.
Trachoma, a chronic follicular conjunctivitis, afflicts an estimated 500 million persons worldwide and has blinded millions, particularly in Africa. The disease is usually con-tracted in infancy or early childhood from the mother or other close contacts. Spread is by contact with infective human secretions, directly via hands to the eye, or via fomites transmitted on the feet of flies.
The prevalence of chlamydial urethral infection in US men and women ranges from 5% in the general population to 20% in those attending sexually transmitted disease clin-ics. Approximately one third of male sexual contacts of women with C. trachomatis cer-vicitis develop urethritis after an incubation period of 2 to 6 weeks. The proportion of men with mild to absent symptoms is higher than in gonorrhea. Nongonococcal urethritis is most commonly caused by C. trachomatis and less frequently byUreaplasma ure-alyticum. Reinfection is common.
PATHOGENESIS
Chlamydiae have a tropism for epithelial cells of the endocervix and upper genital tract of women, and the urethra, rectum and conjunctiva of both sexes. The LGV biovar can also enter through breaks in the skin or mucosa. Once infection is established, there is a release of proinflammatory cytokines such as interleukin-8 by infected epithelial cells. Chlamydial lipopolysaccharides probably also play an important role in initiation of the inflammatory process. This results in early tissue infiltration by polymorphonuclear leukocytes, later followed by lymphocytes, macrophages, plasma cells and eosinophils. If the infection progresses further (because of lack of treatment and/or failure of immune control), aggregates of lymphocytes and macrophages (lymphoid follicles) may form in the submucosa; these can progress to necrosis, followed by fibrosis and scarring.
The chronic sequelae of progressive inflammation with scarring that are seen in trachoma and some female genital tract infections are commonly due to persistent or recurrent infections, which may, in turn, be controlled by host cell immune responses. One theory is that this may result from molecular mimicry, involving epitopes found on the chlamydial 60-kd heat shock protein and also on human cells.
IMMUNITY
C. trachomatis infections do not reliably result in protection against reinfection althoughthere is evidence that secretory immunoglobulin A may confer at least some partial im-munity against genital tract reinfection. Any strain-specific protection that may result is short-lived. Local production of antibody, along with CD4+ lymphocytes of the Th1 type that traffic to the genital mucosa may together play a role in mitigating most acute infec-tions. This would at least partially explain why most untreated chlamydial genital tract in-fections are persistent, but often subclinical in character.
Related Topics