Chapter: Pathology: Female Genital Pathology
Cervix - Pathology
CERVIX
Pelvic inflammatory disease (PID) is an ascending infection
(sexually transmitted disease) from the cervix to
the endometrium, fallopian tubes, and pelvic cavity. The infecting organisms
are most frequently nongonococcal organisms, including Chlamydia, Mycoplasma hominis
and endogenous flora. Broad-spectrum antibiotics are therapeutic.
The distribution of disease
includes the endometrium (endometritis), fallopian tubes (salpingitis), and
pelvic cavity (peritonitis and pelvic abscesses). Fitz-Hugh– Curtis syndrome (perihepatitis) can occur,
characterized by “violin-string” adhe-sions between the fallopian tube and
liver capsule. Symptoms include the following:
•
Vaginal discharge (cervicitis)
•
Vaginal bleeding and midline abdominal pain (endometritis)
•
Bilateral lower abdominal and pelvic pain (salpingitis)
•
Abdominal tenderness and peritoneal signs (peritonitis)
•
Pleuritic right upper quadrant pain (perihepatitis)
Complications of PID include
tubo-ovarian abscess; tubal scarring (increasing risk of infertility and
ectopic tubal pregnancies), and intestinal obstruction secondary to fibrous
adhesions.
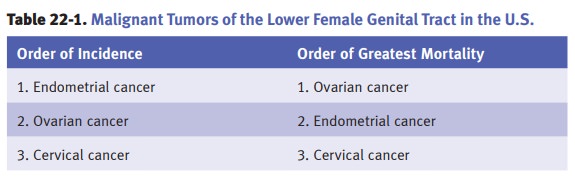
Cervical carcinoma is most
commonly squamous cell carcinoma but can also be adenocarcinoma or small cell
neuroendocrine carcinoma. It is the third most com-mon malignant tumor of the
lower female genital tract in the United States, with peak incidence at ages
35–44. Risk factors include the following:
•
Early age of first intercourse
•
Multiple sexual partners
•
Multiple pregnancies
•
Oral contraceptive use
•
Smoking
•
STDs (including human papilloma virus)
•
Immunosuppression
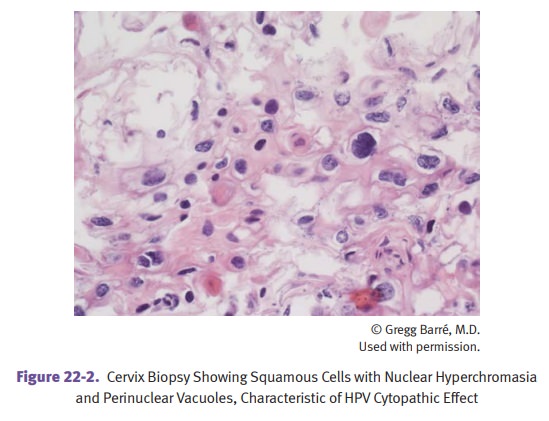
Human papilloma virus infection
is the most important risk factor, with high-risk types being 16, 18, 31, and
33, and having viral oncoproteins E6 (binds to p53) and E7 (binds to Rb).
The precursor lesion is cervical
intraepithelial neoplasia (CIN), which is increasing in incidence and occurs
commonly at the squamocolumnar junction (transformation zone). Cervical
intraepithelial lesions show a progression of changes on histologic
examination:
•
Low grade SIL (squamous intraepithelial lesion)
•
High grade SIL
•
Carcinoma in situ
•
Superficially invasive squamous cell carcinoma
•
Invasive squamous cell carcinoma
Squamous cell carcinoma of the
cervix may be asymptomatic or may present with postcoital vaginal bleeding,
dyspareunia, and/or malodorous discharge. To establish the diagnosis, the
Papanicolaou (Pap) test is useful for early detection, and colpos-copy with
biopsy for microscopic evaluation.
Acute cervicitis and chronic cervicitis are common and
usually nonspecific inflam-matory conditions.
•
Acute cervicitis is often caused by C. trachomatis, N.
gonorrhoeae, T. vaginalis, Candida, and herpes simplex type 2.
•
A specific, severe form of chronic cervicitis (follicular cervicitis) can be caused by
C. trachomatis; it can result in
neonatal conjunctivitis and pneu-monia in infants delivered vaginally through
an infected cervix.
Cervical polyp is a common
non-neoplastic polyp that can be covered with columnar or stratified squamous epithelium.
Related Topics