Chapter: Forensic Medicine: Asphyxia
Causes of asphyxic death: Deaths due to pressure on the neck
Deaths due to pressure on the neck
This group of deaths includes strangulation with
the hands or throttling, strangulation with a ligature, and hanging.
Causes of death
Death is caused by one or more of the following.
Airway obstruction. Direct pressure on the larynx and trachea (throat and windpipe) or
upward displacement of the larynx (throat) against the pharynx can obstruct the
airways. This results in hypoxic-anoxic anoxia.
In a similar manner the base of the tongue may
be displayed backwards against the throat.
Compression of the veins in the neck. Compression of the internal and external
jugular veins (the veins at the side of the neck) prevents blood flow from the
head to the heart. This is especially serious if the carotid arteries are still
open, as blood flow into the head region is still possible, but the blood
cannot flow out of that region. This leads to stagnation of inter alia blood
flow to and from the brain.
Compression of the carotid arteries. This is less common than compression of the
veins, as more pressure is required. This results in stagnation hypoxia.
Compression of the vertebral arteries (the blood vessels running through the
vertebral column to the brain) is rare, as they are protected by bone. With
bilateral compression of the carotid arteries loss of consciousness occurs
almost immediately, as the vertebral arteries are not able to supply sufficient
blood to the brain to preserve consciousness. In elderly individuals pressure
on the carotid arteries may damage the blood vessel walls and atheroma plaques
may be dislodged, which can then cause a stroke.
Neurogenic stimulation. This is a very important cause of death. At the bifurcation of the
carotid arteries in the neck, baro- or pressure receptors are located in a
slight dilation in the blood vessel, the carotid sinus. Usually these receptors
play a role in controlling blood pressure. If the latter rises, the receptors
are stimulated due to the higher pressure in the blood vessels, and via a
reflex arc the heartspeed is then suppressed or inhibited. As the vagus nerve
forms part of this reflex arc, this reflex is also known as the vaso-vagal
response. Mechanical stimulation of these receptors by pressure triggers a
parasympathetic response. The heart rate drops (bradycardia), the person could
faint, and if severe enough, reflex cardiac arrest may occur. Alcohol, hypoxia,
drugs such as cocaine, as well as anxiety and fear can sensitise these
receptors and cause an exaggerated response.
Neurogenic cardiac arrest is more common in
throttling and hanging than in strangulation. The receptors are partially
covered by the neck muscles. During throttling the fingers dig below the
muscles and can stimulate the receptors directly. With hanging the knot in the
cord often lies directly over the receptors. With strangulation with a
ligature, the ligature is usually lower down over the neck, away from the
receptors. Blows to the neck can also stimulate the receptors directly or
indirectly (like in martial arts). In cases of bolus death, branches of the
same nerves supplying these receptors, are stimulated in the back of the
throat, and this causes a similar effect. In some individuals the receptors may
be very sensitive, and even stimulation by the collar of a shirt can cause the
individual to faint.
Combination of the above mechanisms: Throttling is a dynamic process. During the
struggle the grip on the neck is continuously changed. More than one of the
above causes can therefore be involved. It is also important to remember that
hypoxia due to compression of the airways will stimulate the carotid receptors,
and therefore increase the risk of neurogenic cardiac arrest.
Throttling (strangulation with the hands)
Throttling is relatively common, especially in
domestic murders, sex-associated murders and child murders. In order to
overpower and throttle a person, the perpetrator has to have a physical
advantage. Females therefore seldom throttle victims (apart from children) and
even men don't often succumb to throttling. As has been said throttling is a
dynamic process with the hands changing the grip continously. Any of the above
causes of death may therefore occur.
The post-mortem signs are local skin wounds,
caused by the fingers of the assailant as well as those of the victim. The
contusions and abrasions vary in size, and are usually round or oval in shape.
They tend to be present mostly on one side of the neck. The distribution (one
mark on the one side and four marks on the opposite side) could indicate
whether the assailant was left- or right-handed.
Abrasions may be caused by the fingers and nails
of the assailant as well as those of the victim. Many are caused by the victim
himself, in an effort to break the grip of the assailant. It is therefore
important always to examine the nails of the victim, and to collect any
material under the nails. This material can be genetically analysed for
comparison with the genetic profile of the alleged assailant.
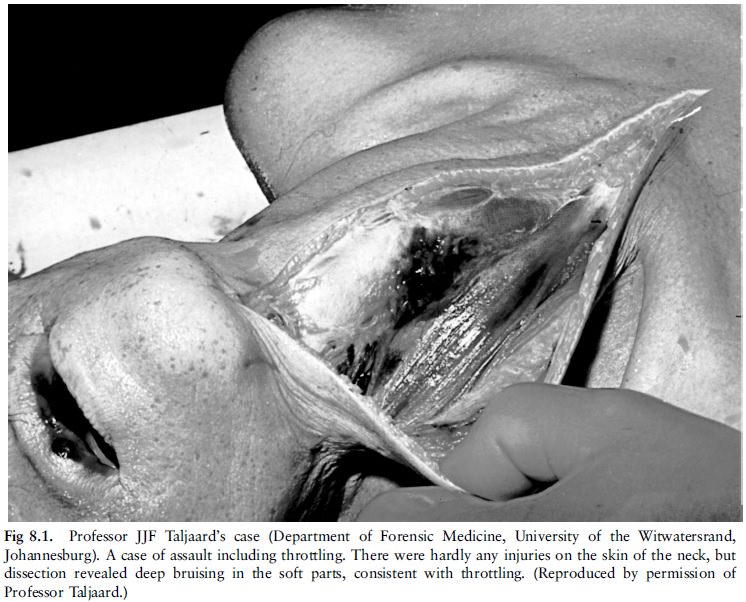
Damage to the deep-lying structures, for
instance haemorrhage into the soft tissue and muscles of the neck, damage of
the vascular structures as well as fractures of the bone and cartilage of the
neck may also occur (fig 8.1). Haemorrhage into the thyroid gland may also
occur.
In cases of death due to violence to the neck,
the neck structures must be examined carefully. Post-mortem extravasation or
leakage of blood during the dissection procedure can easily be confused with
ante-mortem haemorrhage. It is therefore important to use a bloodless field
dissection technique in all cases of suspicious trauma to the neck. The body is
opened with an incision from the suprasternal notch downwards, and the internal
organs are removed. The brain is then removed and a block is placed underneath
the neck to facilitate draining of the blood. The neck is than dissected in a stepwise
manner and all findings noted. Bony structures like the hyoid bone (tongue
bone) are also carefully examined.
Signs of asphyxia are often absent, as the death
is often caused by neurogenic cardiac arrest due to vasovagal inhibition.
Strangulation with a ligature
In this group of deaths the force is applied to
the neck with a ligature or rope. This ligature can be wrapped around the neck,
and can even be knotted. If it is very thin (like fishing line) it can cut into
the skin. It can also be wound up by means of a stick, the so-called Spanish
windlass. In suicide numerous knots and windings may be seen. Strangulation
differs from hanging, as the body weight plays no role.
Strangulation can be the result of an accident
(when a tie is caught in a rotating wheel or lathe), or homicide or suicide.
The post-mortem findings include local skin lesions, mainly a ligature mark (photos 30 and 39). This is an impression abrasion caused by the ligature. Soft material does not necessarily leave any skin wounds. The ligature may be imbedded due to swelling or oedema of the surrounding soft tissue. The mark usually runs horizontally round the neck, relatively low down, just above or below the laryngeal prominence (Adam's apple). There can be scratches on the skin of the neck made by the victim in an effort to release the ligature. There is less damage to the neck structures than in throttling. ``Asphyxia'' signs are petechial haemorrhages and oedema, and they are often pronounced above the ligature.
Neck holds
·
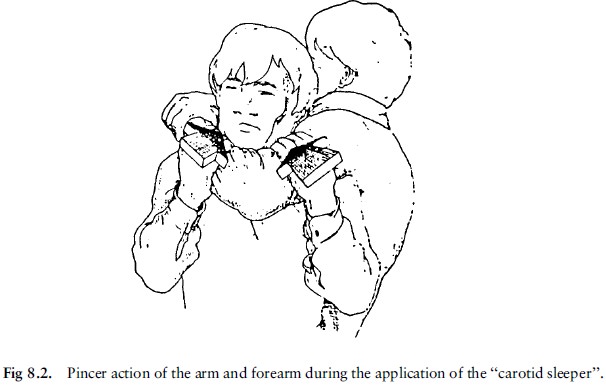
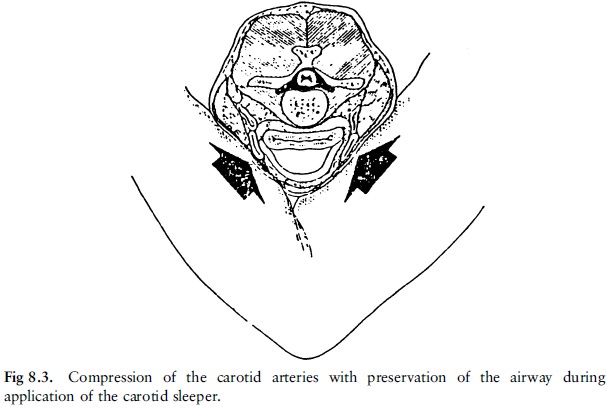
The neck hold grip, also called the ``carotid sleeper'', is a neck hold
used by law enforcement personnel as a means of incapacitating a person during
arrest (figs 8.2 and 8.3). The hold is intended to impede blood flow in the
carotid arteries by pressure on both sides of the neck. This pressure is
applied by the pinching effect of the arm and forearm of the person applying
the hold. If properly applied the airway, including the larynx and trachea,
should be unaffected while the carotid arteries are compressed, and blood-flow
through the vertebral arteries also will not be affected. However, these latter
vessels do not supply sufficient blood to the brain, and this will result in
temporary loss of consciousness. In addition the carotid sinuses containing the
baro-receptors can also be stimulated, causing a reflex action which will
decrease the heart rate and lead to loss of consciousness.
·
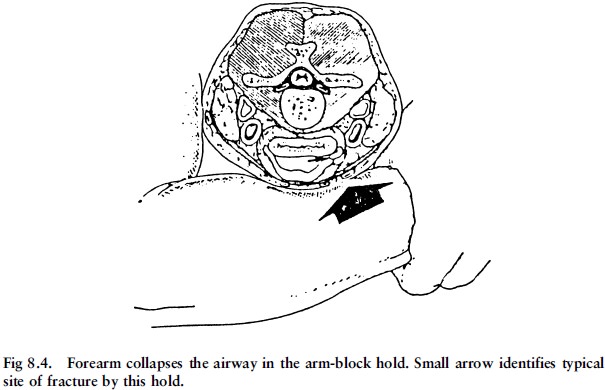
The arm block, or bar arm control, is a hold where the forearm is placed
over the front of the neck and the force is applied backwards, causing
occlusion of the airways. The base of the tongue is also forced back violently
and obstructs the throat. The thyroid cartilage could be damaged. During the
struggle to escape from this hold, the carotid sinus can be stimulated. Damage
to blood vessels can dislodge atherosclerotic plaques causing a fatal stroke.
A properly applied neck hold or carotid sleeper
is generally safe, while arm blocks or bar arm controls could be dangerous.
There are risk factors that can lead to death
during the application of a neck hold:
1)
Men over the age of 40 often have underlying ischaemic heart disease.
Stimulation of the carotid sinus, or hypoxia, can cause an abnormal heart
rhythm, leading to death. In addition damage to atherosclerotic plaques
in the neck arteries can cause a thrombo-embolus
(blood clot), which can lead to a stroke.
2)
Mentally disturbed persons can be extremely violent, displaying
unpredictable behaviour during arrest, so that more force has to be applied
during the struggle, with a subsequent higher risk of fatal hypoxia.
3)
Persons with epilepsy are not only vulnerable to the hypoxia which can
result from such a neck hold, but they could have convulsions or epileptic
seizures during the application of the neck hold, causing more force being
applied to the neck.
4)
Persons under the influence of drugs or alcohol also often display
violent and unpredictable behaviour during an arrest. The resulting struggle increases
the risk of hypoxia
Moreover, the drugs often have a stimulating or
sensitising effect on the carotid sinus, increasing the risk of neurogenic
cardiac arrest.
5)
Certain drugs, such as digitalis and tricyclic anti-depressants, can
cause cardiac arrhythmia (irregular heartbeat), making the heart more
susceptible to hypoxia as well as neurogenic cardiac arrest.
6)
A person who runs away in an effort to escape, is usually out of breath
when arrested. This relative hypoxia, together with the adrenaline which is
secreted in a stress situation, increase the sensitivity of the carotid sinus.
Related Topics