Chapter: Essentials of Psychiatry: Substance Abuse: Caffeine Use Disorders
Caffeine Intoxication
Caffeine Intoxication
Definition
The Diagnostic
and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision
(DSM-IV-TR) defines caffeine in-toxication as a set of symptoms that develop
during or shortly af-ter caffeine use (American Psychiatric Association, 2000).
There may be two kinds of presentation associated with caffeine intoxi-cation.
The first presentation is associated with the acute inges-tion of a large amount of caffeine and represents an
acute drug overdose condition. The second presentation is associated with the chronic consumption of large amounts of
caffeine and results in a more complicated presentation.
The diagnosis of caffeine intoxication is based on
the DSM-IV TR criteria of substance intoxication. Specifically, this disorder
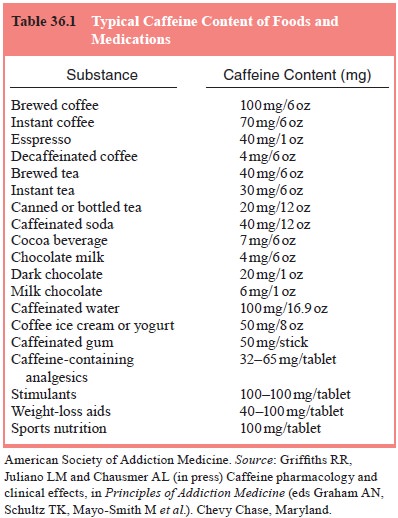
is diagnosed after the consumption of 250 mg of caffeine. Table 36.1 indicates
the approximate caffeine content of numerous foods. This diagnosis is
entertained when at least five of the following 12 signs are present and they
produce significant distress not due to a general medical condition:
·
nervousness
·
restlessness
·
insomnia
·
periods of inexhaustibility
·
dieresis
·
excitement
·
gastrointestinal disturbance
·
muscle twitching
·
psychomotor agitation
·
flushed face
·
tachycardia or cardiac arrhythmia
·
rambling flow of thought and speech
Acquired Tolerance
In a person who regularly consumes caffeine,
tolerance may oc-cur to the acute effects of caffeine. Thus a sensitive person
with no tolerance to caffeine might have signs and symptoms of caf-feine
intoxication in response to a relatively low dose of caffeine (such as 100 mg,
the amount found in a typical cup of brewed coffee) (Table 36.1), whereas
another person with a high daily consumption of caffeine would show no evidence
of intoxication with a similar dose.
Inadvertent Overdosing
Although caffeine intoxication can occur in the
context of ha-bitual chronic consumption of high doses, probably most often it
occurs after inadvertent overdosing. Examples include over-dosing of
intravenous caffeine to children in medical settings (e.g., for respiratory
stimulating effects), excessive caffeine consumption in tablet form by students
who fail to appreciate the dose being ingested (e.g., to study through the
night), and the person who unknowingly consumes a highly concentrated form of
caffeine (e.g., caffeinated coffee brewed with caffeine-containing water to
create an especially high dose of caffeine in the coffee).
Pathophysiology
The principal cellular site of action of caffeine
is the adenosine receptor, where caffeine functions as an antagonist.
Adenos-ine produces a wide variety of physiological effects, including
decreasing spontaneous electrical activity in brain, inhibiting
neurotransmitter release in brain, decreasing spontaneous and operant motor
activity, dilating central vasculature, producing antidiuresis, inhibiting
renin release, and inhibiting gastric se-cretion and lipolysis. As an
antagonist of adenosine many of caf-feine’s actions are opposite to those
produced by adenosine (e.g., central nervous system stimulation, decreased
cerebral blood flow, increased renin release and diuresis, increased gastric
se-cretions and stimulation of respiration).
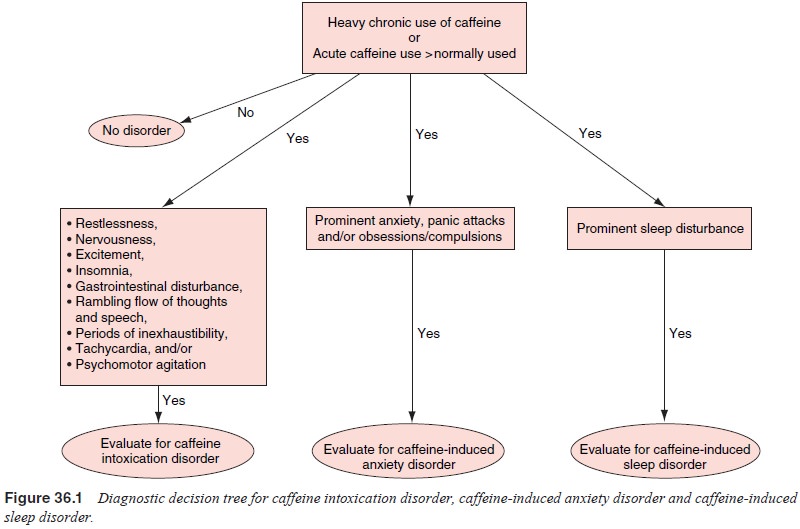
Assessment
The primary features of caffeine intoxication can
be found in the diagnostic criteria from DSM-IV. The diagnostic decision tree
for caffeine intoxication disorder, caffeine-induced anxi-ety disorder and
caffeine-induced sleep disorder is shown in Figure 36.1. The most common
symptoms reported in decreasing order of frequency are frequent urination,
restlessness, insomnia, nervousness and excitement (all which were at rates
greater than 20%). In addition, nearly 25% of people report heart pounding in
response to high caffeine use (although this is not one of the DSM-IV
criteria).
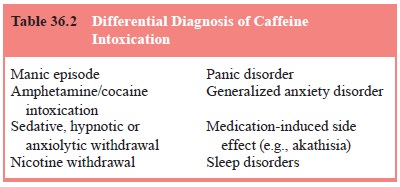
Differential Diagnosis
The diagnosis of caffeine intoxication is based on
the history and clinical presentation of the patient. Ideally, the extent of
caffeine exposure can also be assessed by a serum or saliva assay of the
caffeine level. In the past, caffeine use has often been overlooked in patients
presenting with symptoms consistent with a caffeine use disorder. However, it
may be that there is presently a greater awareness of the deleterious effects
of caffeine, making psychia-trists more sensitive to the inclusion of caffeine
in a differen-tial diagnosis (see Table 36.2), and patients more aware of the
possible role of excessive caffeine in somatic and psychological symptoms.
Epidemiology
Despite the long history of recognition of caffeine intoxica-tion, there is little information available about the prevalence or incidence of caffeine intoxication either in the general commu-nity or in selected populations. It appears that the incidence of caffeine intoxication in the general community is about 7% per year, and it may be higher in selected populations at greater risk for caffeine intoxication (e.g., students).
Course
In the patient who is not tolerant to caffeine,
acute caffeine inges-tion producing caffeine intoxication is a time-limited
condition that will rapidly resolve with cessation of caffeine use, consistent
with the relatively short half-life of caffeine (3–6 hours).
Related Topics