Chapter: Essentials of Psychiatry: Substance Abuse: Caffeine Use Disorders
Caffeine Dependence
Caffeine Dependence
Definition
The clinical features of individuals with caffeine
depend-ence were described in a series of 16 cases described by Strain and
colleagues (1994). Most of these individuals reported physical or psychological
problems from caffeine use which had prompted multiple unsuccessful attempts to
cut down or quit caffeine use, often in response to physicians’
recommendations. Most reported tolerance to caffeine and withdrawal when
attempting to abstain completely. A double-blind withdrawal trial showed
functional im-pairment in most cases. For the group, median daily caffeine
intake was 357 mg with a wide range of 129 to 2548 mg. The preferred ve-hicle
was almost equally divided between soft drinks and coffee.
Etiology
It is known that the consumption of caffeine may be
influenced by several different factors, which are summarized below.
Caffeine Subjective Effects
Many studies have shown that caffeine in low to
moderate doses (20–200 mg) produces mild positive subjective effects of
increased feelings of well-being, alertness, energy, concentra- tion,
self-confidence, motivation for work and desire to talk to people. The profile
of positive effects with caffeine is qualita-tively similar to that produced by
d-amphetamine and cocaine, which may
reflect a common dopaminergic mechanism of action. High doses of caffeine
(e.g., 800 mg) produce negative subjec-tive effects such as anxiety and
nervousness, especially in people who are not tolerant to caffeine.
Caffeine Reinforcement
Consistent with its ability to produce mild
positive subjective ef-fects, low to moderate doses of caffeine have also been
shown to function as a reinforcer in humans, that is, when given the choice
under experimental conditions, some people will consistently choose to consume
caffeine rather than placebo.
Caffeine Tolerance
Survey data indicate 17% of current caffeine users
reported toler-ance (Hughes et al.,
1998), whereas 75% of a group of caffeine dependent individuals reported
tolerance (Strain et al., 1994).
Although tolerance is one of the criteria for making a diagnosis of caffeine
dependence (see DSM-IV-TR criteria for substance dependence), it is not clear
what role the development of toler-ance may have in the development of clinical
dependence upon caffeine.
Genetics and Caffeine Use
Genetic studies suggest that caffeine use problems
have an un-derlying biological basis, part of which may be shared with other
commonly abused substances. Twin studies comparing monozy-gotic and dizygotic
twins showed heritabilities of heavy caffeine use, caffeine tolerance and
caffeine withdrawal which ranged be-tween 35 and 77% (Kendler and Prescott, 1999).
Caffeine Use and Alcoholism
The conclusion suggested by the genetic studies
described above is that a common genetic factor underlies joint use of
caffeine, alcohol and cigarettes. This is consistent with findings of studies
on the cooccurrence of use of these three substances (Kozlowski et al., 1993). A study of individuals
whose pattern of caffeine use fulfilled
DSM-IV diagnostic criteria for substance dependence on caffeine found that
almost 60% had a past diagnosis of alcohol abuse or dependence (Strain et al., 1994).
Caffeine Use and Nicotine/Cigarette Smoking
Epidemiological studies have shown that cigarette
smokers con-sume more caffeine than nonsmokers (Swanson et al., 1994).
Caffeine Use in Psychiatric Patients
Surveys of psychiatric patients (typically
inpatients) have found high rates of caffeine consumption, particularly among
patients with schizophrenia. Other groups at risk may include substance abusers
(Russ et al., 1988; Hays et al., 1998) and patients with
an-orexia nervosa (Sours, 1983). While preliminary work suggests there may be
some factors (such as heritability) that contribute to the predisposition to
use caffeine, there are no studies that have examined the possible etiologic
role of such factors in the devel-opment of caffeine dependence as a specific
diagnosis. Caffeine dependence, like other drug dependence syndromes, in all
likeli-hood represents the interaction of social and cultural forces, and
individual histories and predispositions, operating in the context of a
psychoactive substance that produces pleasant subjective ef-fects and is
reinforcing.
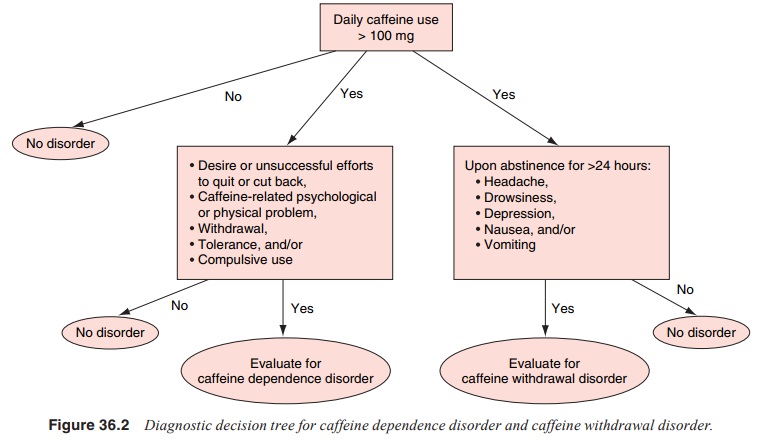
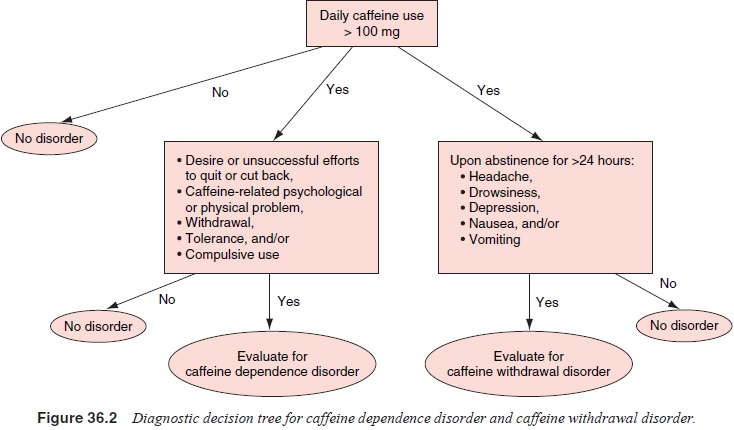
Assessment
Caffeine dependence may be an unrecognized
condition with a higher prevalence than is generally appreciated (see Figure
36.2). Clinicians do not typically think to inquire about caffeine use and
about problematic use consistent with a diagnosis of caf-feine dependence.
However, probing for evidence of caffeine dependence may be useful, and it
would be reasonable to focus upon the DSM-IV criteria for dependence that are
more appro-priate for a substance that is widely available and generally
cul-turally accepted. Thus, the clinician should probe for evidence of
tolerance, withdrawal, continued use despite a doctor’s rec-ommendation that the
person cut down or stop using caffeine, use despite other problems associated
with caffeine, often using larger amounts or over a longer period than
intended, or per-sistent desires and/or difficulties in decreasing or
discontinuing use.
Differential Diagnosis
The diagnosis of caffeine dependence includes
symptoms that can also contribute to a diagnosis of caffeine intoxication and
caffeine withdrawal, and both of these conditions should be included in the
differential diagnosis of a patient with possible caffeine dependence. Since
intoxication and withdrawal symp-toms can contribute to the diagnosis of
dependence, conditions that overlap with these caffeine-related disorders
should also be considered. When considering a patient for a possible diagnosis of
caffeine dependence, the clinician should also consider other substance
dependence syndromes – especially those related to stimulants – in the
differential diagnosis
Epidemiology
Caffeine
is the most widely used mood-altering drug in the world. In North America,
dietary surveys indicate that weekly or more frequent consumption of
caffeine-containing foods occurs in 80 to 90% of children and adults (Gilbert,
1984; Hughes and Oliveto, 1997). In the USA, average daily caffeine consumption
among caffeine consumers is 280 mg (Barone and Roberts, 1996). There is only
one study of the prevalence of caffeine dependence in the general population
based upon standardized diagnostic criteria (Hughes et al., 1998). In this random telephone survey of residents of Vermont,
162 out of the 202 surveyed participants reported current caffeine use.
Employing the generic DSM-IV criteria for dependence, 30% of the 162 current
caffeine users fulfilled criteria for a diagnosis of caffeine dependence by
endorsing three or more dependence criteria, with 56% endorsing the diagnostic
criterion of persistent desire or unsuccessful efforts to cut down or control
caffeine use, 28% endorsing using more than intended, 14% endorsing caffeine
use continued despite knowledge of a physical or psychological problem likely
to have been caused or exacerbated by caffeine use, 18% endorsing withdrawal
and 9% endorsing tolerance. These results suggest there may be a large number
of people who demonstrate symptoms consistent with a DSM-defined diagnosis of
caffeine dependence.
Course
While there are no studies that have specifically
examined the course and natural history of caffeine dependence, like other drug
dependence syndromes caffeine dependence appears to be a chronic relapsing
disorder. In the study described above by Strain and colleagues (1994),
caffeine dependence participants reportedrecurrent efforts to discontinue
caffeine use, with failures to dis-continue use or frequent relapses.
Treatment
In a survey of physicians’ practices, it was found
that over 75% of medical specialists recommend that patients reduce or
elimi-nate caffeine for certain conditions including anxiety, insomnia,
arrhythmias, palpitations and tachycardia, esophagitis/hiatal hernia and
fibrocystic disease (Hughes et al.,
1988). However, stopping caffeine use can be difficult for some people. For
exam-ple, in the diagnostic study of caffeine dependence (Strain et al., 1994), subjects reported
physical conditions such as acne rosa-cea, pregnancy, palpitations and gastrointestinal
problems that led physicians to recommend that they reduce or eliminate
caf-feine; all reported that they were unable to follow their doctors’
recommendations
Related Topics