Chapter: Modern Medical Toxicology: Chemical Poisons: Non-Metallic Chemical Poisons
Bromine - Chemical Poisons
Bromine
Bromine
is a dark reddish-brown, heavy liquid with irritant brown fumes. By itself it
is rarely encountered in poisoning cases, while the salts (bromides) have often
been implicated, especially in the past when they were used extensively in
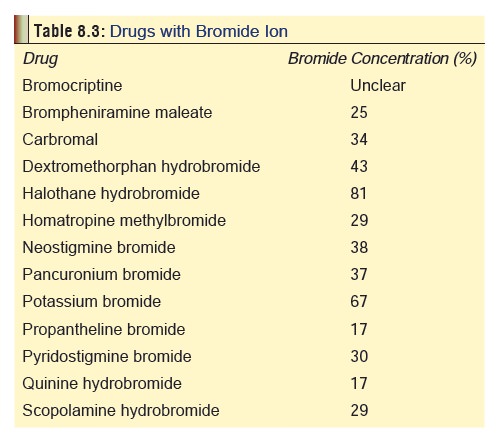
therapeutics as sedative-hypnotics. Even today there are several therapeutic
drugs (many of them over-the-counter preparations) which contain bromide ion
and have the potential for chronic toxicity (Table 8.3). Methyl bromide is used in soil fumigation which can
result in bromide levels as high as 380 mg/kg in vegetables such as lettuce,
spinach, tomatoes, radishes, and cucumbers among others. Ethylene dibromide is
used in the posthar-vest fumigation of warehouses, ships’ holds, and quarantine
chambers affecting fruits, wheat, almonds, tobacco, and dried mushrooms;
achieving levels as high as 300 mg/kg.
Usual Fatal Dose
Blood
bromide level of 300 mg/100 ml is potentially lethal. Levels greater than 50 to
100 mg/100 ml are usually associated with signs and symptoms of toxicity.
Acceptable
daily intake: 1 mg/kg.
Clinical Features
·
Bromine is extremely corrosive to
the eyes, skin, bronchial tree and mucous membranes in liquid or vapour form.
·
Ingestion may cause severe corrosive
injury to the gastro-intestinal mucosa, abdominal pain, haemorrhagic
gastro-enteritis, and circulatory collapse.
·
Inhalation causes respiratory tract
irritation, cough, bron-chospasm, upper airway oedema and delayed pulmonary
oedema.
·
Ocular exposure results in
irritation, lacrimation, inflam-mation, blepharospasm and photophobia.
·
Skin contact causes burns with brown
discolouration and slowly healing ulcers.
·
Acute poisoning with bromides causes
severe gastrointestinal
·
irritation with nausea and vomiting,
which usually prevents absorption of large doses.
·
Methyl bromide or ethylene dibromide
inhalation provokes cough, dyspnoea, pneumonitis, pharyngitis, and pulmonary
oedema. Eye exposure results in conjunctivitis and keratitis. Dermal contact
produces redness and blistering. Ingestion results in headache, vertigo,
vomiting, diarrhoea, metabolic acidosis, ventricular fibrillation, convulsions,
and hepato-renal damage.
·
When therapeutic drugs containing
bromides are taken for a long period, chronic poisoning results refered to as bromism:
o Anorexia,
nausea, salty taste, halitosis, lassitude, low-grade fever, drowsiness,
amnesia, slurred speech, abnormal gait, tremor, nystagmus, visual disturbances,
and psychosis. Impotence and loss of libido have been reported.
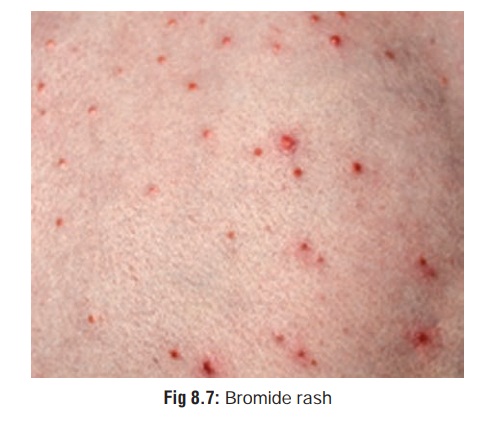
o Bromide
rash is sometimes seen, which is an acneiform eruption beginning in the face
and spreading gradu-ally to the rest of the body (Fig 8.7). It may progress to pustular lesions and ulceration (bromodermatuberosum).

·
Bromides cross the placenta and may
be detected in the milk of nursing mothers. Case reports suggest that prenatal
exposure may cause growth retardation, craniofacial abnor-malities and
developmental delay.
Diagnosis
·
Urine
test: Add 5 ml chloroform and a few drops of nitricacid to 10 ml
urine. Allow to stand for 3 minutes. A yellow chloroform layer is diagnostic
for bromide intoxication.
·
Decreased anion gap.
·
Serum bromide level: more than 100
mg per 100 ml is significant.
·
Bromides are often radiopaque. Abdominal
x-ray may be helpful in confirming diagnosis of acute ingestion and detecting
bezoar formation.
Treatment
1. Acute Poisoning—
·
Milk or water can be administered as
a first-aid measure.
·
Activated charcoal in the usual
manner (for organic bromide compounds).
·
Treatment of convulsions with
diazepam or phenytoin or babiturates.
·
Decontamination of skin and eye.
·
Sodium chloride orally or
intravenously (vide infra).
·
Supportive measures.
·
Haemodialysis in severe cases.
Chronic Poisoning—
·
Stop bromide ingestion.
·
Oral or intravenous sodium chloride.
It promotes excre-tion of bromides. Discontinue when symptoms have improved,
and the serum bromide level is less than 100 to 150 mg/dL Administration of
diuretics such as furosemide (10 mg IV, 4th or 6th hourly) can improve bromide
clearance.
·
If saline administration is
contraindicated for any reason, administer ammonium chloride, or undertake
haemodialysis.
Related Topics