Chapter: Surgical Pathology Dissection : Breast
Breast Lumpectomy : Surgical Pathology Dissection
Lumpectomy
Lumpectomy for a Grossly Benign Palpable Mass
A
lumpectomy specimen from a palpable mass that is grossly benign should be
measured, inked, and serially sectioned perpendicular to the clos-est palpable
margin. Inspect the cut surface and record the size and appearance of the
lesion as well as its distance from the margins. Sequen-tially submit the
entire lumpectomy specimen in up to 10 cassettes. Be sure that your sections
show the border of the lesion with the surrounding breast tissue (important for
distinguishing fibro-adenoma from phyllodes tumors), and take perpendicular
sections from the lesion to the margins. If the margins are designated, be sure
to obtain a section perpendicular to each of the six margins. Cost-effective
strategies for handling large lumpectomy specimens have also been proposed.
Schnitt et al.11,12 suggested submit-ting a maximum of 10 initial
sections of the fibrous tissue in these cases, as carcinoma and atypical
hyperplasia are unlikely to be found in the fatty tissue alone.
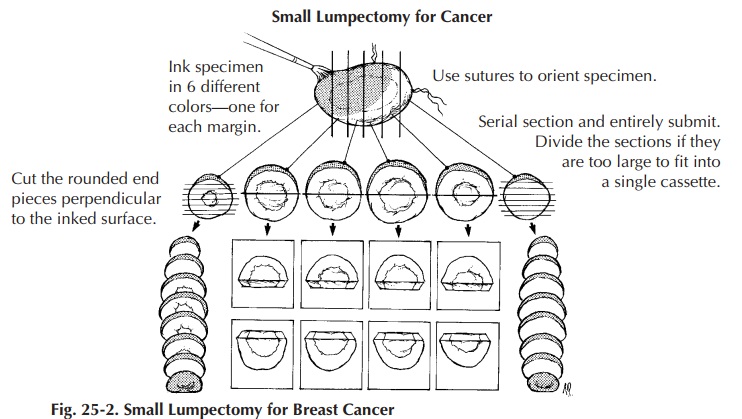
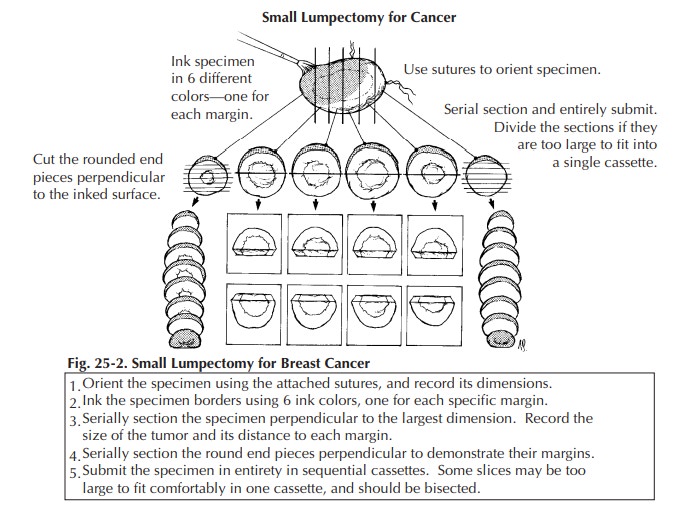
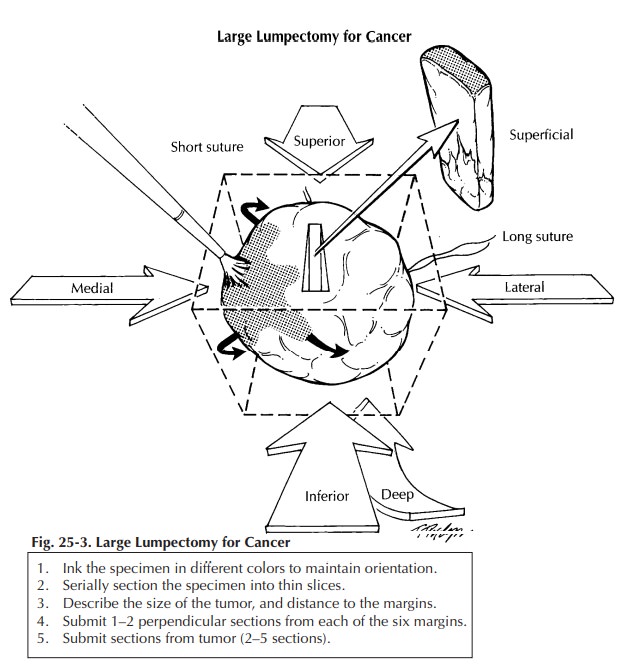
Lumpectomy for Grossly Identifiable Cancers
Lumpectomy biopsies for grossly identifiable cancers are usually brought to the surgical pathology laboratory with some indication of orientation provided by the surgeon. Frequently, but not universally, a short stitch is used to desig-nate the superior aspect of the specimen and a long stitch to designate the lateral aspect of the specimen. From these two landmarks you can then determine the inferior, medial, anterior, and posterior margins. As illustrated, these margins are easier to conceptualize if you think of the specimen as a cube. After orienting the speci-men, measure it, ink it, and obtain one or two perpendicular sections from each of the six mar-gins (superior, inferior, medial, lateral, superfi-cial, deep). Serially section the specimen at 2- to 3-mm intervals. Note the size of the tumor and the distance to each of the margins. Obtain two to five sections of the tumor. If a portion of skin is present, it should also be sampled for histologic examination. If the lumpectomy specimen is rela-tively small, submit it entirely (Figure 25-2). For large lumpectomy specimens, where the entire specimen cannot be submitted in 20 cassettes, submit representative sections (Figure 25-3).
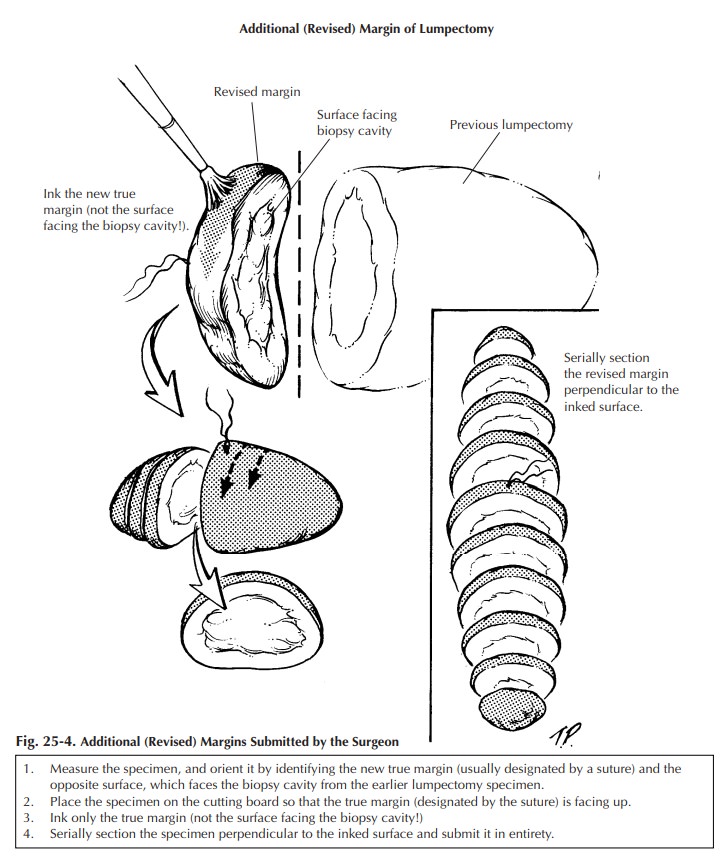
Additional (Revised) Margins Submitted by the Surgeon
Sometimes
the surgeon separately submits addi-tional (revised) margins for one or all six
of the lumpectomy surfaces. Usually these specimens appear as a strip of tissue
with a stitch on one face marking the new margin. The opposite sur-face, which
would face the lumpectomy speci-men, often contains fresh blood and is not a
true margin. Ink the surface containing the stitch, obtain serial sections
perpendicular to the ink, and submit all of the sections for microscopic
examination (Figure 25-4). Do not ink the oppo-site surface; otherwise, it may
be impossible to tell which is the true margin.
Re-excision Lumpectomy
Re-excision
lumpectomies are generally per-formed because a positive margin was identified
during a prior excision. Therefore, specimen sam-pling should focus on the
biopsy cavity to docu-ment the presence of residual disease and on the new
specimen margins to ensure the adequacy of tumor removal during the
re-excision. Try to submit re-excision specimens in their entirety if they can
be submitted in fewer than 10 cassettes. If the biopsy cavity appears grossly
benign, two sections per centimeter of greatest specimen diameter is probably
adequate.
Related Topics