Chapter: Surgical Pathology Dissection : Bone, Soft Tissue, and Skin
Bone : Surgical Pathology Dissection
Bone
General Comments
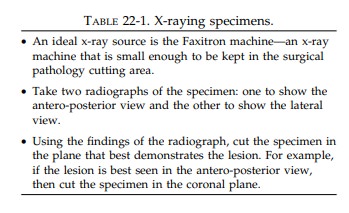
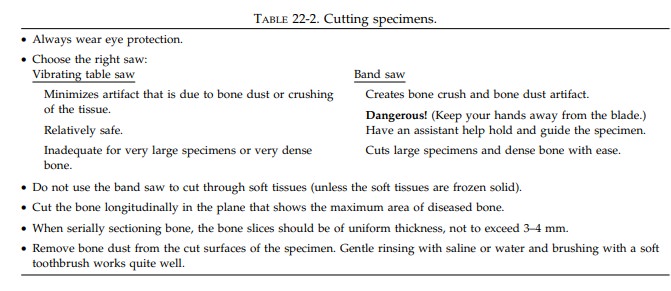
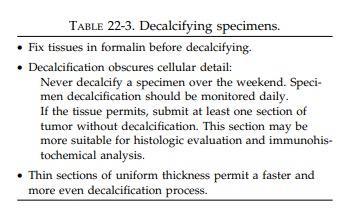
The hardness of bone introduces three challenges that are unique to the dissection of bone speci-mens: (1) Many lesions involving bone are not easily appreciated simply by palpating and inspecting the intact specimen. This inability to pinpoint the lesion may frustrate attempts to demonstrate its size and location when cutting the bone specimen. (2) Bone specimens cannot be easily dissected and sampled with standard knives and scalpels. (3) Since the microtome blade also cannot penetrate bone, bone cannot easily be sectioned in the histology laboratory. Fortu-nately, each of these obstacles can be overcome. Specimen radiographs (Table 22-1) allow one to visualize the extent and location of the patho-logic process so that the specimen can be cut in the proper plane; appropriate saws (Table 22-2) allow one to cut bone without destroying the speci-men; and finally, special solutions (Table 22-3) can demineralize bone making it easier to sec-tion for microscopic evaluation. Thus, the success-ful dissection of bone specimens requires that the prosector master the use of radiography, special techniques, instruments, and a variety of chemical solutions.
Small Bone Fragments
Whether
dealing with bone biopsies, currettings, or the removal of small bones, there
is always the danger of overdecalcifying the tissue. Efforts to minimize the
time in decalcification solution and to separate out tissue fragments that do
not require decalcification will reap great rewards when evaluating these
tissues microscopically. When it is necessary to cut a bone fragment before
processing, orient and cut the bone to show as much surface as possible. For
example, small tubular bones such as metatarsals or ribs should be cut
longitudinally rather than in cross section. When articular cartilage is
present, sections should be taken to show its relationship to cortical bone.
For specimens consisting of multiple pieces of tissue, soft tissues should be separated
from bone and processed routinely in formalin without decalcification, while
pieces of bone should be grouped in cassettes ac-cording to size and density to
allow for uniform decalcification.
Large Bone Specimens
Femoral heads are the most common example of large bone specimens. They are usually removed because of either osteoarthritis or a hip fracture. Consequently, it is particularly important to identify, inspect, and sample the articular surface and any fracture site.
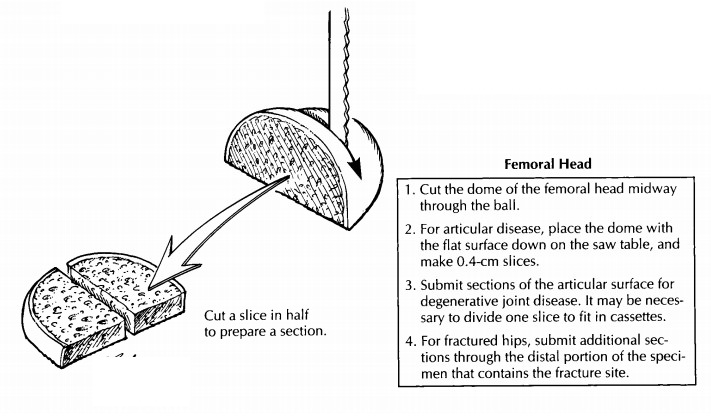
Measure the specimen and describe the articular cartilage,
noting whether it is eroded, frayed, pitted, or absent. The presence of
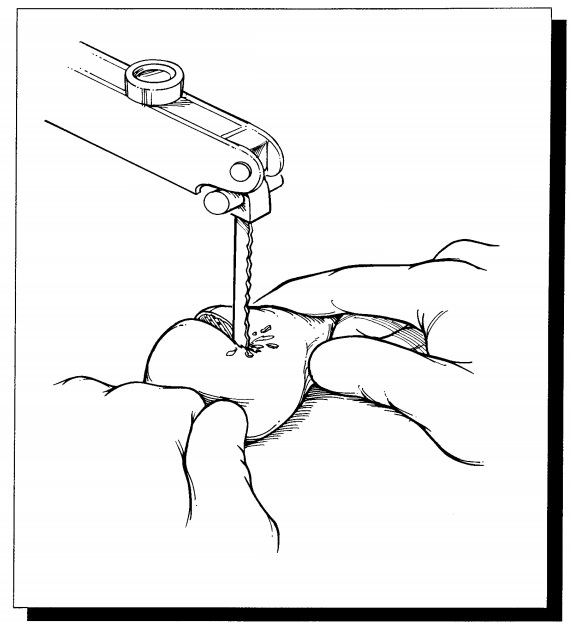
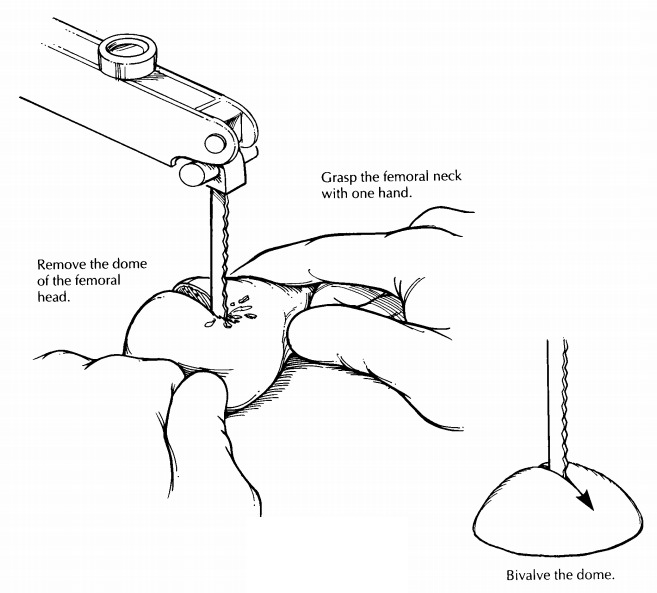
osteophytes should also be noted. As illus-trated, separate the dome of the
femoral head from the neck, then place the cut surface of the head on the table
saw, and section it into 4-mm slices in a plane perpendicular to the articular
cartilage. Note the density of the bone and the thickness of the cartilage. In
a similar manner, serially section the femoral neck. Look for the presence of
blood clot, marrow hemorrhage, or a neoplasm.
Sampling for histology should be guided by the clinical history and gross findings. For cases of osteoarthritis, sample the femoral head to show cartilage destruction and the reaction of the un-derlying bone. In cases of fracture, direct your attention to the fracture site; most of the sections should come from this area. Always submit at least one cassette of soft tissue including the syno-vial membrane and capsule.
Segmental Resections and Amputations for Neoplasms
Segmental Resections
Segmental
resections of bone are performed for malignant neoplasms and aggressive benign
tumors. Because local recurrence is an important complication, the margins of
resection need to be carefully evaluated. The soft tissue margins are best
sampled while the specimen is intact and still easy to orient. After inking the
soft tissue resection margin, sample the margin using per-pendicular sections
from those areas for which there is gross or radiologic suspicion of margin
involvement.
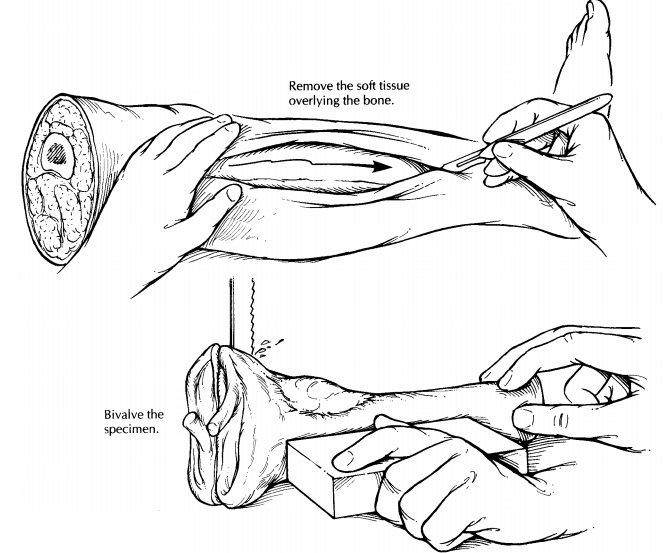
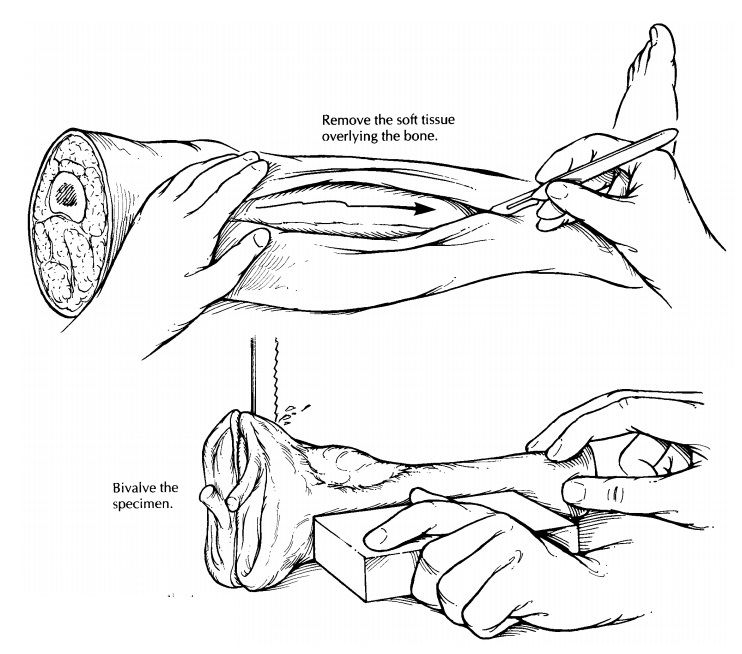
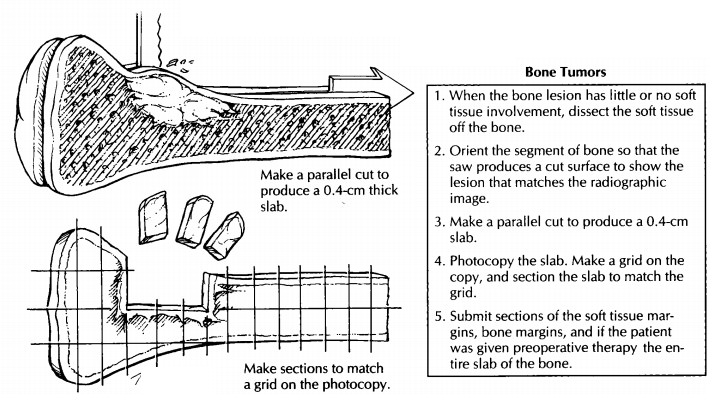
After soft tissue margins are sampled, decide which plane of section will best demonstrate the lesion. The radiographic findings will help guide this strategy. For the saw to cleanly pass through the bone, expose the surfaces of the bone as illustrated by cutting through and peeling back the soft tissues in this plane. Next, bisect the bone in the appropriate plane (usually the coronal plane) using a band saw. Inspect the cut surface. The extent of the lesion should then be measured and described. In addition, the presence of corti-cal penetration and soft tissue extension should be noted. Look for noncontiguous ‘‘skip’’ lesions in the medullary canal, and measure the distance from the edges of the tumor to the bone resection margin. Scoop a small amount of marrow from the end(s) of the bone, and submit this marrow as the bone margin(s).
An
alternative method is to freeze the entire specimen. The frozen specimen does
not re-quire removal of the soft tissues before cutting the bone. Thus, the
relationship of the bone neo-plasm to soft tissue spread is better preserved.
Now you
are ready to cut a slab from the face of the bone cut surface. Place one half
of the bisected specimen on the band saw, and cut a complete 4-mm-thick slab,
then photograph and x-ray the slab. Ideally, this slab should be thin, uniform,
and represent the greatest surface area of the tumor. Before sectioning the
slab further, make a representation of the slab to map the precise location of
each section submitted for his-tology. One method is to photocopy the slab and
then to draw grids slightly smaller than your cassette size on the photocopy.
The entire slab can then be blocked out and submitted for micro-scopic
examination according to the grids on the photocopy.
When the
patient has received neoadjuvant chemotherapy, the entire face of the slab
should be evaluated microscopically to determine the percentage of tumor
necrosis. When the patient has not received neoadjuvant chemotherapy, you may
be more selective in the sections that you submit for histology. Important
areas that should always be sampled include: (1) the intramedul-lary component
of the neoplasm; (2) penetration of the tumor through the cortex; (3) extension
of the tumor into soft tissues; (4) the interface of the tumor with normal
bone; (5) involvement by the tumor of an articular surface and/or joint space;
and (6) the bone margin(s).
Amputation Specimens
Although
amputations for tumor appear more complex than segmental resections as a result
of their size and bulk, they can be dissected along the same guidelines given
for segmental resections. Indeed, after margins are sampled, the portion of the
limb containing the bones and joints not involved by the neoplasm can be
removed. This, in essence, converts the specimen to one that is similar to the
segmental resection.
Important Issues to Address in Your Surgical Pathology Report on Bone Tumors
· What
procedure was performed, and what structures/organs are present?
· What
type of neoplasm is present?
· What are
the size and histologic grade of the neoplasm?
· If the
patient received neoadjuvant chemo-therapy, what is the percentage of tumor
necrosis?
· Is there
any cortical penetration or soft tissue invasion?
· What is
the status of the soft tissue and bone margins of resection?
·
Is a skip lesion present?
Related Topics