Chapter: Surgical Pathology Dissection : Bone, Soft Tissue, and Skin
Soft Tissue : Surgical Pathology Dissection
Soft Tissue
Soft
tissue resections are often complex speci-mens containing soft tissues, skin,
and sometimes even bone. The general approach to these speci-mens is a simple
one, and it parallels that outlined for complex head and neck specimens, identify
the various components of the specimen (soft tissue, bone, and skin). Second,
think of each component as a geometric shape. Third, approach each component
separately. Fourth, look for relationships between any le-sions and each
component.
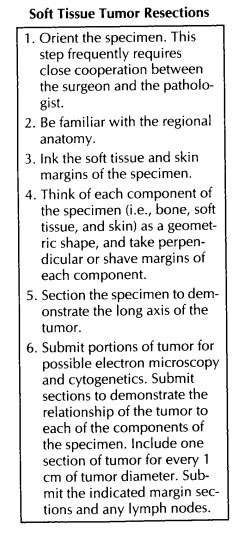
With the
general approach outlined above in mind, start the dissection by orienting the
speci-men. Do not hesitate to ask the surgeon to help with this step. Large
muscle bundles move easily relative to one another. A margin that looks close
in fact may have been covered by a large bundle of muscle that has shifted. The
only way to be sure that tissue has not shifted is to discuss the speci-men
with the surgeon. Next, make sure that you know the anatomy. The origin of a
sarcoma from a nerve can be missed if one is not familiar with the anatomic
location of the major nerves in the specimen. After the specimen has been
oriented and the anatomy determined, identify the various components of the
specimen (soft tissue, bone, skin, etc.). This step helps ensure that important
components of the specimen are not left out of the dissection.
Next,
measure the overall dimensions of the specimen, and document the size of each
indi-vidual component. The external appearance of each component can then be
described. In partic-ular, note the size and position of any biopsy sites.
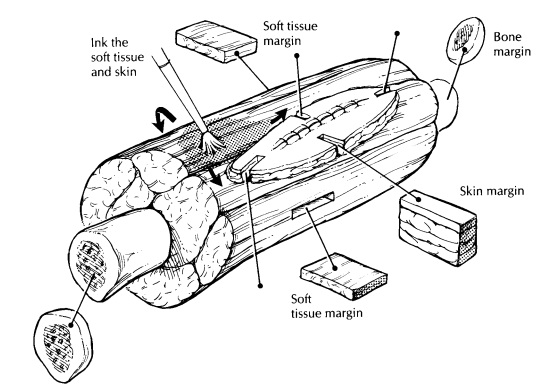
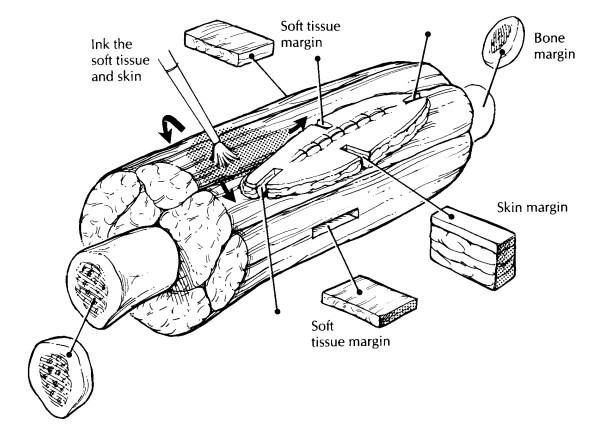
The next
step is to sample the margins. The evaluation of the margins of a large complex
specimen is simplified by thinking of each com-ponent of the specimen as a
geometric shape. As illustrated, the soft tissue can usu-ally be thought of as
a cube, the bone as a cylin-der, and, if present, the skin as a square sheet.
Ink the specimen, and take sections to demon-strate the margins of each of the
components. It may be impractical to ink the entire specimen, but the closest
margins (identified visually or by palpation) should be inked. There are
usually six soft tissue margins (a cube has six sides), and these can be taken
as perpendicular margins. These margins usually include the anterior,
posterior, medial, lateral, inferior, and superior surfaces. Similarly, there
are usually four skin margins (a square has four sides), and these can be taken
as perpendicular margins. If a margin consists of a fascial layer, periosteum,
or other anatomic barrier such as the diaphragm, this should be specified. The
bone (the ends of a cylinder), vascular, and neural margins can be taken as
parallel (shave) sections, but perpendic-ular rather than en face margins are
suggested in general.
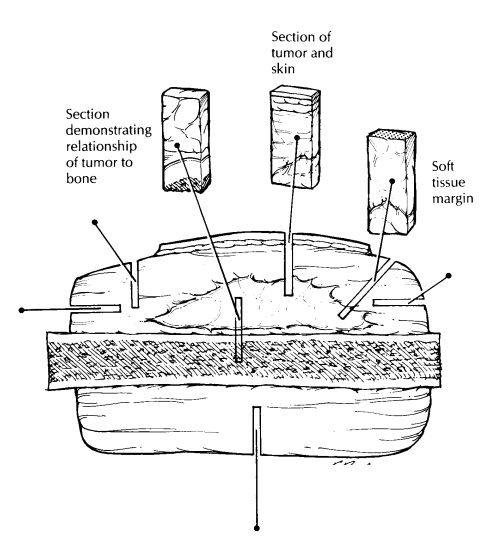
The
specimen can now be sectioned. Determine the location and long axis of the
tumor by palpat-ing the specimen and reviewing the preoperative computed
tomography (CT) scans. Section the specimen using a long sharp knife in the
plane that will demonstrate the largest cross section of the tumor. Carefully
document the size (try to give three dimensions), consistency, and color of the
tumor. Measure twice, because size is one of the most important predictors of
outcome for patients with a soft tissue tumor. It is im-portant to document the
epicenter of the tumor (e.g., dermal, subcutaneous, fascial, subfascial,
intramuscular, visceral, or a combination). Also note whether the tumor is
centered on or extends into major vessels, nerves, or joint spaces. These
features are important for staging and for identi-fying the site of origin of
the tumor. Also note any cysts and areas of necrosis (estimate the percent if
necrosis is identified), hemorrhage, calcification, myxoid change, bone
formation, or cartilage, and whether the edge of the tumor is encapsu-lated,
pushing, or infiltrative. It may be helpful to correlate the gross appearance
of the tumor with radiographic findings. For example, if calci-fications are
seen in a particular area of the tumor on CT scan, then that area should be
identified grossly.
Next,
document the distance of the tumor to each of the margins and the relationship
of the tumor to each of the various components of the specimen. It is important
to measure margins that are less than 2 cm from the tumor. Areas where the
margins are more than 5 cm clear need not be sampled (except in cases of
angiosarcoma or epithelioid sarcoma, which are prone to sub-clinical satellite
spread). Document the number of lymph nodes present, and sample each for
histology. Lymph nodes may not be included, as only a small number of sarcoma
types are likely to have lymph node deposits (e.g., angiosarcoma, epithelioid
sarcoma, synovial sarcoma, clear cell sarcoma).
Finally,
the tumor itself can be sampled. First, submit a representative piece in
glutaraldehyde for possible electron microscopy. Next, as clini-cally
indicated, submit fresh tissue for cytogenet-ics or other special studies.
These studies may be particularly important in the pediatric pa-tient. Finally,
submit sections for routine histology. These should include sec-tions that
demonstrate the relationship of the tumor to each component of the specimen,
sec-tions that demonstrate the relationship of the tumor to the closest
margins, and sections from any foci within the tumor that look different from other
areas of the tumor. A useful rule of thumb is that one section should be
submitted for every 1 cm of the maximum diameter of the tumor. As you take
these sections, keep in mind that important indications of tumor grade
(cellularity, necrosis, mitoses, etc.) and differen-tiation may be present only
focally in large masses.
Important Issues to Address in Your Surgical Pathology Report on Soft Tissue Tumors
• What procedure was performed, and what
structures/organs are present?
• What are the size, type, and histologic
grade of the neoplasm?
• Does the neoplasm extend into skin,
muscle, periosteum, bone, a joint space, major vessels, or major nerves?
• Are any margins involved? List distance
from margins closer than 2 cm.
• Are there any satellite lesions?
• Is there evidence of metastatic disease?
Re-cord the number of lymph nodes examined and the presence or absence of lymph
node metastases.
Related Topics