Chapter: Modern Pharmacology with Clinical Applications: Antipsychotic Drugs
Antipsychotic Drugs: Pharmacology
PHARMACOLOGY
Phenothiazines are classified
on the basis of their chem-istry, pharmacological actions, and potency.
Chemical classifications include the aliphatic (e.g., chlorproma-zine; Thorazine), piperidine (e.g.,
thioridazine; Mellaril), and
piperazine subfamilies. The piperazine derivatives are generally more potent
and pharmacologically se-lective than the others. The thioxanthenes (e.g.,
thio-thixene; Navane) are chemically
related to the pheno-thiazines and have nearly equivalent potency.
Thebutyrophenone haloperidol (Haldol)
is structurally dis-tinct from the two preceding groups, offering greater
potency and fewer autonomic side effects. The dibenzo-diazepine clozapine (Clozaril) bears some structural
re-semblance to the phenothiazine group but causes little extrapyramidal
toxicity. The benzisoxazole risperidone (Risperdal)
is representative of many of the newer agents in having a unique structure
relative to the older groups while retaining antipsychotic potency and a
bet-ter side effect profile.
Pharmacokinetics
Most of the antipsychotics
are readily but incompletely absorbed, and many undergo significant first-pass
me-tabolism. The oral bioavailability of chlorpromazine and thioridazine is in
the range of 25 to 35%, while that of haloperidol, which is less likely to be
metabolized, has an oral bioavailability of about 65%. The antipsychotics are
highly lipid soluble and are about 95% bound to pro-teins. Generally they have
a much longer clinical dura-tion of action than could be estimated from their
plasma half-lives; this is likely due to their sequestration in fat tissue.
Depot preparations are more slowly absorbed and longer acting, and thus can be
administered par-enterally at intervals up to 3 weeks. The main routes of
metabolism are mediated by hepatic oxidative microso-mal enzymes and by
glucuronidation. Some metabolites, such as 7-hydroxychlorpromazine, retain
measurable ac-tivity, but this effect is not considered to be clinically im-portant;
an exception to this observation is the major metabolite of thioridazine, which
is more potent than the parent drug. Since drug blood concentrations of the
less potent antipsychotics are lower after several weeks of treatment at the
same dose, it is believed that these compounds may weakly induce their own
metabolism. Also, the ability to metabolize and eliminate these drugs has been
shown to diminish with age. Typical elimination half-lives vary from 12 to 24
hours.
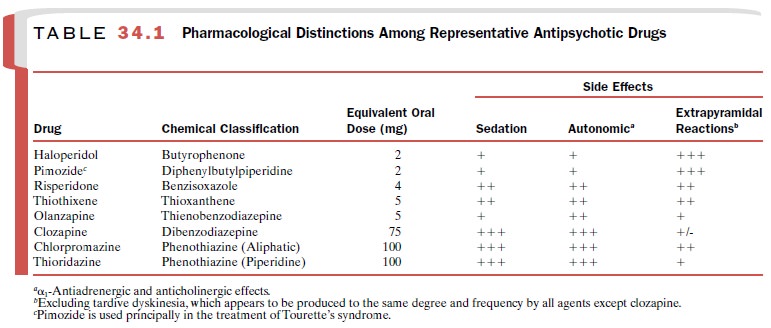
Pharmacological Distinctions
Despite differences in
potency, all commonly used an-tipsychotic drugs have approximately equal
efficacy in equivalent doses. However, individual patients may be more
responsive to one drug class than another. Prototype or representative members
of the antipsy-chotics are arranged in decreasing order of potency in Table
34.1. While the sedative and autonomic effects of the high-potency drugs are
less prominent, these agents are more likely to cause acute extrapyramidal
symp-toms. Generally, these trends are reversed as potency decreases.
All antipsychotics block D2-receptors,
but the de-gree of blockade in relation to actions on other recep-tors varies
greatly. For example, chlorpromazine andthioridazine block α-adrenoceptors (autonomic
side effects) more potently than D2-receptors and also block 5-HT2
serotonergic and H1 histamine receptors (sedative side effects) to a
significant extent. However, their affinity for D1-receptors is
weak. Haloperidol and pimozide (Orap)
act mainly on D2-receptors (ex-trapyramidal toxicity) with
negligible activity at D1-receptors. Clozapine, risperidone, and
olanzapine (Zyprex) show marked
clinical differences from the other drugs. Clozapine binds more to D4,
5-HT2, α1-, and H1-receptors (autonomic and sedative side
effects) than to either D2 (low extrapyramidal activity) or D1
sites. Risperidone binds primarily to D2-, 5-HT2-, and α1-receptors, retaining high
potency with lesser potential for side effects. Current drug development is
directed toward a search for atypical antipsychotics like clozap-ine that have
a broad spectrum of effects on other neu-rotransmitter receptors.
Other Pharmacological Actions
Antipsychotic drugs produce
shifts in the pattern of electrographic (EEG) frequencies, usually slowing them
and causing hypersynchrony. This slowing is sometimes focal or unilateral,
which may pose diagnostic problems, but the frequency and amplitude changes are
readily ap-parent. The hypersynchrony produced by these drugs probably accounts
for their activating effect on the EEG in epileptic patients and for the low
incidence of seizures in patients with no history of seizure disorders.
Antipsychotics produce
striking effects on the re-productive system. Amenorrhea and increased libido
have been reported in women, whereas decreased li-bido and gynecomastia have
been observed in men. Some of these actions are undoubtedly the result of a
drug-associated blockade of dopamine’s tonic normal inhibition of prolactin
secretion, but they may also be partially due to an enhanced peripheral
conversion of androgens to estrogens.
Orthostatic hypotension and
high resting pulse rates can result from the use of the low-potency
phenothi-azines. Mean arterial pressure, peripheral resistance, and stroke
volume are decreased, while pulse rate is in-creased. Abnormal
electrocardiograms (ECGs) have been observed, especially following thioridazine
admin-istration. These findings include prolongation of the QT interval and
abnormal configurations of the ST segment and T waves, the latter being rounded,
flattened, or notched. These effects are readily reversed upon drug withdrawal.
Related Topics