Chapter: Essential Clinical Immunology: Immune Regulation
Antibodies and Other Immunosuppressive Methods
ANTIBODIES AND OTHER IMMUNOSUPPRESSIVE METHODS
There are a number of instances in which antibodies
have been used to suppress the immune response. Among the earliest measures
has been the use of anti-RHD anti-bodies to prevent hemolytic disease of the
newborn due to incompatibility between the mother (RHD−) and an RHD+ fetus. The disease is prevented
by the adminis-tration of anti-D antibodies to the mother immediately after
delivery. This inhibitsthe formation of anti-D antibodies in the mother,
thereby avoiding the development of serious disease in the infant. This
thera-peutic measure has virtually eliminated the incidence of RH disease in
developed countries.
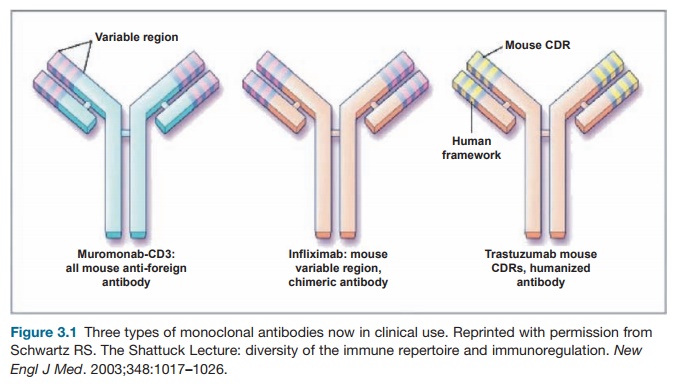
More recently, monoclonal antibodies are being used
to suppress the immune system, and several antibodies are now approved for the
treatment of autoimmune diseases. These antibodies are typically “humanized”
mouse monoclonals, created by transposing the mouse antigen-binding sites onto
a human antibody framework (see Figure 3.1). This technique retains the full
range of effective properties of human Fc while minimizing the immunogenicity
of the mouse component. Antibodies that target the immune system can target
cell surface molecules on T or B cells or can target soluble mediators of
inflammation such as cytokines. Among the most effec-tive uses of monoclonal
antibodies has been in treating severe rheumatoid arthri-tis, using monoclonal
antibody directed against tumor necrosis factor (TNF-α). The drawback to this therapy is that the infusions must be repeated
frequently to sustain results.
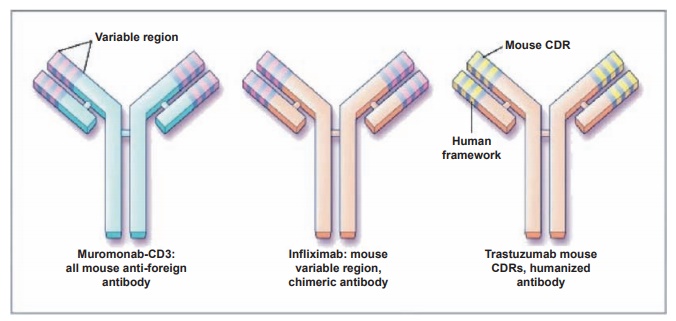
Figure 3.1 Three types of monoclonal antibodies now in clinical use. Reprinted with permission from Schwartz RS. The Shattuck Lecture: diversity of the immune repertoire and immunoregulation. New Engl J Med. 2003;348:1017–1026
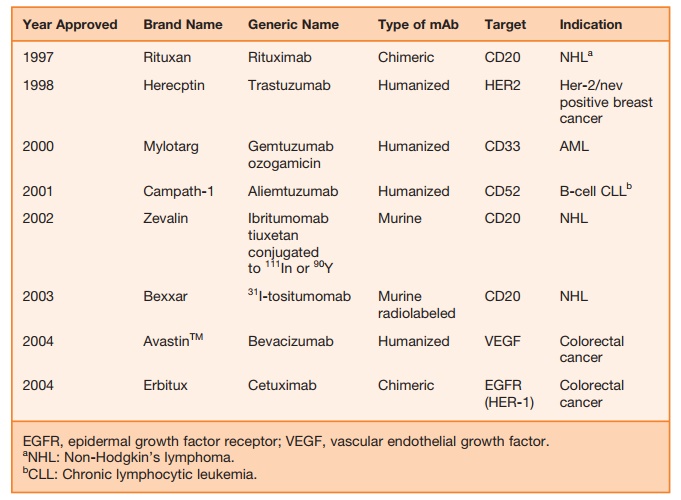
Monoclonal antibodies can also be used as antitumor
agents (see review by Reichert). Specific targeting and killing of tumor cells
can be enhanced by linking tumor antigen-specific monoclonal antibodies to
agents as follows: (1) a cytotoxic drug such as metho-trexate, (2) a
radioisotope such as iodine-131 or ytrium-90, or (3) a toxin such as ricin.
Monoclonal antibodies are now approved for the treatment of non-Hodgkin’s
lym-phoma, myeloid and lymphocytic leuke-mia, breast cancer, and colorectal
cancer (Table 3.2).
Table 3.2 Immunosuppressive Drugs in Clinical Use or Clinical Trials
Some new studies, still in clinical trials, are
occurring in the treatment of prostate cancer, especially metastatic bone
lesions, and it is hoped many more monoclonal antibodies will be forthcoming
against var-ious other tissues.
Other methods of immunosuppression are plasmapheresis or plasma exchange. In the first method, improvement may be due to
removal of mediators of tissue damage, whereas in plasma exchange, it may be
due to replacement of deficient factors or to
Total
lymphoid irradiation produces
long-term suppression of helper T cells and has been used in some severe
autoimmune diseases like lupus or rheumatoid arthritis. The side effects of
this treatment may be severe and sometimes fatal.
Related Topics