Chapter: Clinical Anesthesiology: Anesthetic Management: Anesthesia for Orthopedic Surgery
Anesthesia for Total Knee Replacement
TOTAL KNEE REPLACEMENT
Preoperative Considerations
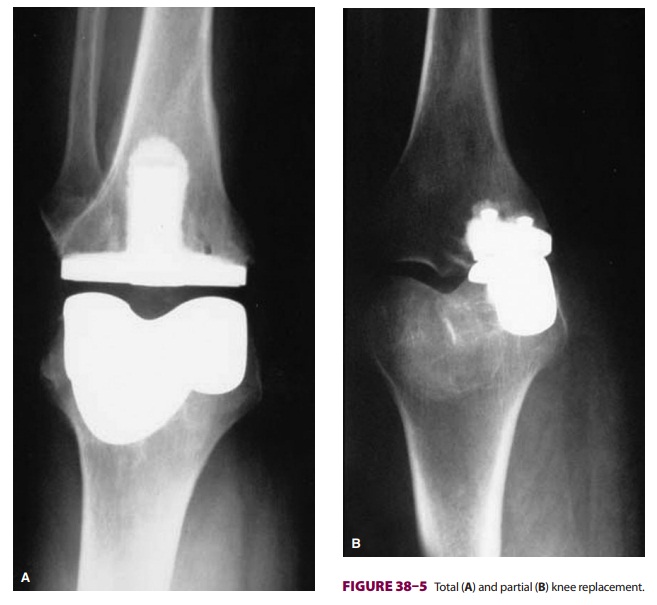
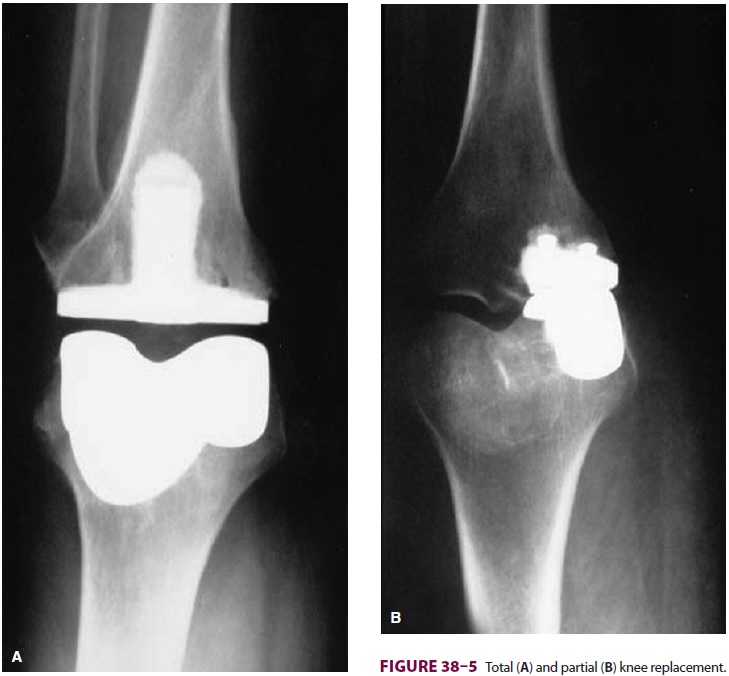
Patients presenting for total knee replacement (Figure
38–5) have similar comorbidities to those undergoing total hip replacement
(eg, RA, osteoarthritis).
Intraoperative Management
During total knee arthroplasty, patients remain in a supine position,
and intraoperative blood loss is limited by the use of a tourniquet.
Cooperative patients usually tolerate a neuraxial anesthetic technique with
intravenous sedation. Bone cement implantation syndrome following insertion of
a femoral prosthesis is possible but is less likely than during hip arthroplasty.
Subsequent release of emboli into the systemic circulation may exaggerate any
tendency for hypotension following tourniquet release.
Preoperative placement of a lumbar epidural or perineural catheter can
be very helpful in
managing postoperative pain, which is
typically more severe than pain following hip replacement surgery. Eff ective
postoperative analgesia facil-itates early physical rehabilitation to
maximizepostoperative range of motion and prevent joint adhesions following
knee replacement. It is impor-tant to balance pain control with the need for an
alert and cooperative patient during physical therapy. Epidural analgesia is
useful in bilateral knee replace-ments. For unilateral knee replacement, lumbar
epidural and femoral perineural catheters provide equivalent analgesia while
femoral perineural catheters produce fewer side effects (eg, pruritus, nausea
and vomiting, urinary retention, or ortho-static lightheadedness). Preoperative
placement in a “block room” can prevent operating room delays and ensure that patients
receive this beneficial anal-gesic technique (Figure 38–6).
Partial knee replacement (unicompartmental or patellofemoral) and minimally invasive knee arthroplasty with muscle-sparing approaches have been described. With strict patient selection, these techniques may reduce quadriceps muscle damage, facilitating earlier achievement of range-of-motion and ambulation goals, and may allow for discharge within 24 h following surgery if outpatient physical therapy is arranged. Anesthetic management and postoperative analgesia should accommodate and facilitate the accelerated recovery schedule. Single or continuous peripheral nerve blocks, alone or in combination, can provide target-specific pain control and facilitate early rehabilitation. In ran-domized clinical trials, continuous peripheral nerve block catheters with subsequent perineu-ral local anesthetic infusions have been shown to decrease time to meet discharge criteria for total knee arthroplasty. The management of peri-neural catheters takes a hands-on team approach and can be incorporated into integrated clinical pathways involving surgery, nursing, and physi-cal therapy. Among the complications of lower extremity perineural local anesthetic infusions, those involving patient falls are of greatest con-cern, and comprehensive fall prevention programs need to be in place wherever these techniques are employed.
Related Topics