Chapter: Clinical Anesthesiology: Anesthetic Management: Anesthesia for Orthopedic Surgery
Anesthesia for Fracture of the Hip
FRACTURE OF THE HIP
Preoperative Considerations
Most patients presenting for hip fractures are frail and elderly. An
occasional young patient will have sustained major trauma to the femur or
pelvis. Studies have reported mortality rates following hip fracture of up to
10% during the initial hospital-ization and over 25% within 1 year. Many of
these patients have concomitant diseases such as coro-nary artery disease,
cerebrovascular disease, chronic obstructive pulmonary disease, or diabetes.
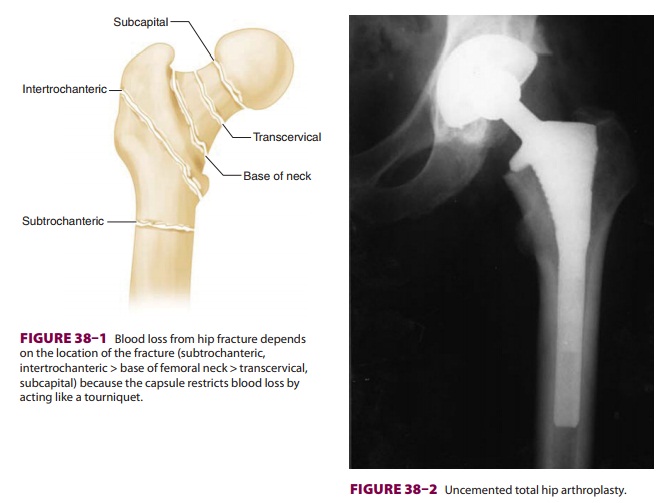
Patients presenting with hip fractures are fre-quently dehydrated from
inadequate oral intake. Depending on the site of the hip fracture, occult blood
loss may be significant, further compromis-ing intravascular volume. In
general, intracapsular (subcapital, transcervical) fractures are associated
with less blood loss than extracapsular (base of the femoral neck,
intertrochanteric, subtrochanteric) fractures (Figure 38–1). A
normal or borderline-low preoperative hematocrit may be deceiving when
hemoconcentration masks occult blood loss.
Another characteristic of hip fracture patients is the frequent presence
of preoperative hypoxia that may, at least in part, be due to fat embolism;
other factors can include bibasilar atelectasis from immobility, pulmonary
congestion (and effusion) from congestive heart failure, or consolidation due
to infection.
Intraoperative Management
The choice between regional (spinal or epidural) and general anesthesia has been extensively evalu-ated for hip fracture surgery. A meta-analysis of 15 randomized clinical trials showed a decrease in postoperative DVT and 1-month mortality with regional anesthesia, but these advantages do not persist beyond 3 months. The incidence of postop-erative delirium and cognitive dysfunction may be lower following regional anesthesia if intravenous sedation can be minimized.
A neuraxial anesthetic technique, with or with-out concomitant general
anesthesia, provides the additional advantage of postoperative pain control. If
a spinal anesthetic is planned, hypobaric or iso-baric local anesthesia
facilitates positioning since the patient can remain in the same position for
both block placement and surgery. Intrathecal opioids such as morphine can
extend postoperative analge-sia but require close postoperative monitoring for
delayed respiratory depression.
Consideration should also be given to the
type of reduction and fixation to be used. This is dependent on the fracture
site, degree of displacement, preop-erative functional status of the patient,
and surgeon preference. Undisplaced fractures of the proximal femur may be
treated with percutaneous pinning

or cannulated screw fixation with the patient in the supine position. A
hip compression screw and side plate are most often employed for
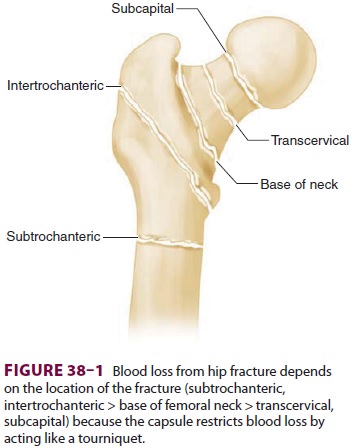
intertrochanteric fractures. Displaced intracapsular fractures may require
internal fixation, hemiarthroplasty, or total hip replacement (Figure
38–2). Surgical treatment of
extracapsular hip fractures is accomplished with either an extramedullary
implant (eg, sliding screw and plate) or intramedullary implant (eg, Gamma
nail).
Hemiarthroplasty and total hip replacement are longer, more invasive
operations than other proce-dures. They are usually performed with patients in
the lateral decubitus position, are associated with greater blood loss, and,
potentially, result in greater hemodynamic changes, particularly if cement is
used. Therefore, one should secure sufficient venous access to permit rapid
transfusion.
Related Topics