Chapter: Maternal and Child Health Nursing : Prenatal Care
Abdominal examination - General examination of the ante-natal patients
Abdominal examination
Aims: To observe signs of pregnancy,
to assess fetal sign andgrowth, To assess fetal health, to detect any deviation
from normal, to diagnose the location of fetal parts.
Preparation:
1.
Ensure that patient empties her bladder
2.
Let the patient lie in the supine position on the
couch, with one pillow under her head. Her arms should be by her sides to
prevent traction of abdominal muscles.
3.
Draw the screen in order to ensure privacy.
4.
Talk to the patient nicely to aid relaxation.
5.
The examiner’s arms and hands should be relaxed.
Three
ways of obtaining information required are: - Inspection, palpation,
Auscultation
Inspection: note the size and shape of the
abdomen
a. Size: Should correspond with the
supposed period of gestation.
If much
larger or smaller:-
·
Review the date of the last normal menses
·
Note the size of the patient. If dates are correct
but uterus is large, possibilities are: multiple pregnancy, polyhydramnios, a
large fetus, a fetus plus uterine fibroid.
b. Shape: Should be longitudinally ovoid.
This is clear in mostprimigravidae.
Round: is due to multiparity, transverse
lie, obesity,polyhydramnios.
In
addition to the above, note on inspection: Pigmentation, scars, striae
gravidarum, The quality of the muscles of abdomen and the contour.
c. Fetal Movement: This is
evidence that the fetus is alive. It alsoaids in the diagnosis of position as
the back will be on the opposite side where movement is seen.
d. Contour of the abdomen: (a)
Normal is dome –shape (b)Pendulous abdomen is common with multigravid woman.
(c) when lightening has taken place the uterus sag forward and uterus is more
prominent e.g. when standing. (d) Depression at the umbilical level suggest
occipito posterior (e) skin-scar, stiae gravidarum, Linea Nigera are observed.
Palpation;
Aim
·
To observe signs of pregnancy. To determine fundal
height Size and growth of the fetus. This should correspond with the period of
gestation.
·
To ascertain fetal parts of the fetus is in
different parts of the uterus, also the lie and attitude of the fetus.
·
Relationship of presenting part to the pelvis: how
to palpate the uterus. Detect any deviation from normal.
The hands
should be clean and warm, cold hands do not have necessary acute sense of touch
and tend to induce contraction of the abdominal muscles. Arms and hands should
be relaxed and the pads NOT THE TIPS of the fingers are used with delicate
precision moving smoothly over the abdomen without lifting them. Erratic and
sudden pressure and rough manipulation are irritating and can cause
contractions making detection of fetal parts impossible.
Abdominal
palpation is done by the following maneuvers: (though not by mean the order)
·
Estimation of fundal height
·
Fundal palpation – To determine the part of the fet
us in the fundus.
·
Lateral palpation
·
Pelvic palpation (lower pole palpation)
Fundal height:
Method: The ulnar border of the left hand
is placed at theupper border of the fundus in order to locate the highest point
of the fundus. As many fingers of the left, hand as can be accommodated are
laid flat between the upper border of the fundus and the xiphisternum. The
distance between fundus and xiphisternum is estimated in fingers breadth. At 36
weeks gestation no fingers can be inserted.
Using MC
Donald’s technique – A measuring tape tha t has centimeter is used. After
locating the fundal height, the zero end of the tape is paced on the symphysis
pubic and stretched to the height of fundus. The measurement on the tape is
recorded as the fundal height. It is more accurate between 20-31 weeks
gestation.
Fundal palpation: This
manoeuvre will help to determinewhether the presentation is cephalic or breech
and the lie longitudinal or transverse. In 95% of cases the breech will be in
the fundus and this denotes a cephalic presentation. When the head is in the
fundus, the presentation is breech. While facing the woman’s head “walk” up
both hands, one o n either side of the uterus and lay them flat on the fundus
of the uterus to feel what is lying there.
Lateral Palpation: This
maneuver is useful to locate thefetal back as an aid to diagnosis of position.
Method: while still facing the patient’s
head or feet, thehands are placed on both sides of the uterus at about
umbilical level. Pressure is applied with the palms of alternate hands to
differentiate the degree of resistance between the two sides of the uterus. One
hand is used to steady the uterus and press the fetus over towards the
examining hand which determines the presence of the broad resistant back or the
small parts that slip under the examining fingers.
By using
a rotary movement of the fingers:
·
The back may be mapped out as a continuous smooth
resistant mass from the breech down to the neck.
·
The limbs are noted as small irregularities which
are often felt to move.
Pelvic palpation: This is
the most important maneuver inabdominal palpation because of its value in the
diagnosis of presentation of the fetus, engagement of its fetal head and
disproportion between head and pelvis. It should not cause discomfort to the
women.
Method: The midwife stands on the
patient’s right with herthighs against the couch, her body, turned at the
waist, facing towards the women’s feet. Using both hands, the midwife finds out
what is in the lower pole of the uterus as follows:
The sides
of the uterus, just below the umbilical level are grasped snugly between the
palms of the hands, the fingers held close together, pointing downwards and
inwards. What ever is in the lower pole can then be held between both hands. In
most cases it is the head that is in the lower pole and is recongised as
follows:
·
It is smooth, round and hard.
·
It is ballotable (if not engaged).
·
It is separated from the trunk by a groove (the
neck)
Occasionally
it is the breech; which is
·
Less hard
·
More irregular
·
The lower limbs are nearer to it.
Pawlik’s grip
This
method of palpating the lower pole of the uterus is most effective when the
head is not engaged.
Method: The midwife, standing on the
patient’s right, faces thewoman’s head and using the right hand, grasps the
lower pole of
the
uterus with the thumb on the woman’s right side and the fingers on the left
side of the uterus. Fingers and thumb must be sufficiently far apart to
accommodate the fetal head.
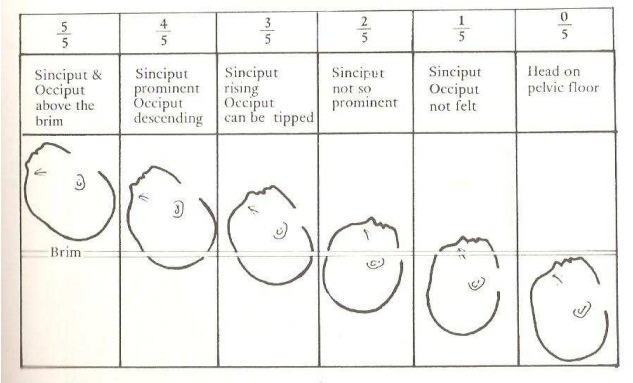
Engagement of the head
Definition
Engagement
means when the widest diameter of the presenting part has passed through the
pelvic brim. In some women engagement does not take place before term. In some
African women it occurs during the first stage of labour.
Recognition of engagement
·
The head or breech is not mobile
·
Less of the head will be felt per abdomen
Auscultation
The fetal
heart sounds are like the ticking of a watch under a pillow. The rate may be
double that of the mother’s heart beast observed at the wrist. About 140 beat
per minute.
Procedure
Place
Pinard’s stethoscope over the back of the fetus and support with the pinna of
the ear while the right hand feels maternal pulse at her wrist.
NOTE: All information obtained must be considered
in making diagnosis. If any information does not correspond, repeat and think
again.
Related Topics