Chapter: Obstetrics and Gynecology: Uterine Leiomyoma and Neoplasia
Uterine Leiomyomas
Uterine
Leiomyomas
Uterine leiomyomata (also called fibroids and myomas) U represent localized proliferation of smooth muscle cellssurrounded
by a pseudocapsule of compressed muscle fibers. The highest prevalence occurs during the fifth decade of
a woman’s life, when they may be present in 1 in 4 white women and 1 in 2 black
women. Uterineleiomyomata are clinically
apparent in 25% to 50% of women, although studies in which careful pathologic
examination of the uterus is carried out suggest that the prevalence may be as
high as 80%. Uterine fibroids vary in size, from microscopic tolarge
multinodular tumors that literally fill the patient’s abdomen. Leiomyomata are
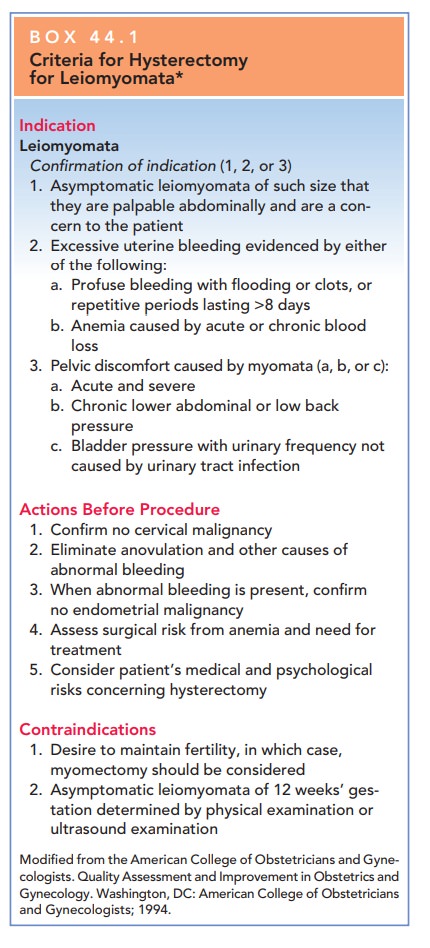
the most common indication for hysterectomy, accounting for approximately 30%
of all such cases. Additionally, they account for a large number of more
conservative operations, including myomectomy, uterine curettage, operative
hysteroscopy, and uterine artery embolization (UAE).
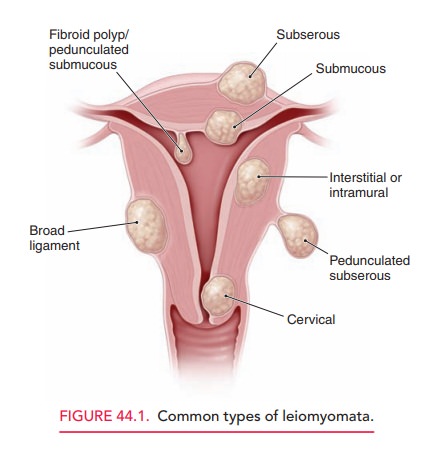
Leiomyomata are classified into
subgroups based on their anatomic relationship to the layers of the uterus. Thethree most common types are intramural (centered in the mus-cular
wall of the uterus), subserosal(
just beneath the uterine serosa), and submucosal
( just beneath the endometrium). Asubset of the subserosal category is the pedunculatedleiomyoma, which appears on
stump-like structures. Mostleiomyomata initially develop from within the
myometrium as intramural leiomyomata. Roughly 5% of uterine myomas originate
from the cervix. Rarely, leiomyomata may occur without evidence of a uterine
origin in places such as the broad ligament and peritoneal cavity. Leiomyomata
are considered hormonally responsive, benign tumors, because estrogen may
induce their rapid growth in high-estrogen states, such as pregnancy. In
contrast, menopause gener-ally causes cessation of tumor growth and even some
atro-phy. Estrogen may work by stimulating the production of progesterone
receptors in the myometrium. In turn, pro-gesterone binding to these sites
stimulates the production of several growth factors, causing the growth of
myomas. Although exact mechanisms are unknown, chromosomal
translocations/deletions, peptide growth factor, and epi-dermal growth factor
are implicated as potential pathogenic factors of leiomyomata. Sensitive DNA
studies suggest that each myoma arises from a single smooth muscle cell and
that, in many cases, the smooth muscle cell is vascular in origin.
The uterine smooth muscle may
also develop a rare cancer, such as leiomyosarcoma.
These are not thought to represent “degeneration” of a fibroid, but, rather, a
new neoplasm. Uterine malignancy is more
typical in postmenopausalpatients who present with rapidly enlarging uterine
masses, postmenopausal bleeding, unusual vaginal discharge, and pelvic pain. An
enlarging uterine mass in a postmenopausal patientshould be evaluated with
considerably more concern for malignancy than one found in a younger woman.
These heterologous, mixed tumors contain other sarcomatous tis-sue elements not
necessarily found only in the uterus.
Related Topics