Chapter: Obstetrics and Gynecology: Uterine Leiomyoma and Neoplasia
Symptoms of Uterine Leiomyomas
SYMPTOMS
Bleeding is the most common
presenting symptom in uterine fibroids. Although the kind of abnormal bleeding
may vary, the most common presentation includes the development of
progressively heavier menstrual flow that lasts longer than the normal duration
(menorrhagia, defined as menstrual
blood loss of >80 mL). This bleeding may result from significant distortion
of the endometrial cavity by the underlying tumor. Three generally accepted but
unproved mechanisms for increased bleeding include:
·
Alteration of normal myometrial
contractile function in the small artery and arteriolar blood supply
under-lying the endometrium
·
Inability of the overlying
endometrium to respond to the normal estrogen/progesterone menstrual phases,
which contributes to efficient sloughing of the endo-metrium
·
Pressure necrosis of the
overlying endometrial bed, which exposes vascular surfaces that bleed in excess
of that normally found with endometrial sloughing
Characteristically, the best
example of leiomyoma con-tributing to this bleeding pattern is by the so-called
sub-mucous leiomyoma. In this
variant, most of the distortioncreated by the smooth muscle tumor projects
toward the endometrial cavity, rather than toward the serosal surface of the
uterus. Enlarging intramural fibroids likewise may contribute to excessive
bleeding if they become large enough to significantly distort the endometrial
cavity.
Blood loss from this type of
menstrual bleeding may be heavy enough to contribute to chronic iron-deficiencyanemia and, rarely, to
profound acute blood loss. Theoccurrence of isolated submucous (subendometrial)
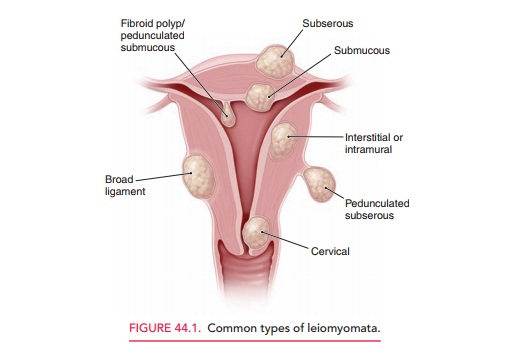
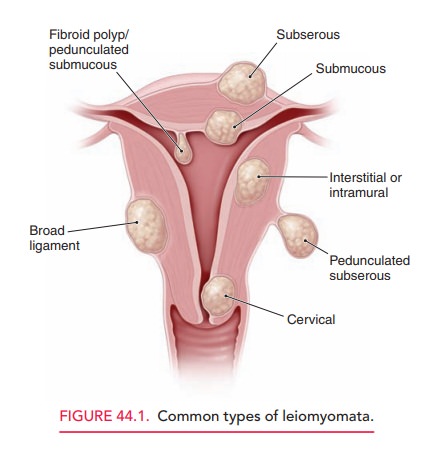
leiomy-omata is unusual. Commonly, these are found in association with other
types of leiomyomata (Fig. 44.1).
Another
common symptom is a progressive increase in “pelvic pressure.” This may
be a sense of progressive pelvicfullness, “something pressing down,” and/or the
sensation of a pelvic mass. Most commonly, this is caused by slowly enlarging
myomas, which on occasion may attain a mas-sive size. These leiomyomata are the
most easily palpated on bimanual or abdominal examination and contributes to
characteristic “lumpy-bumpy,” or cobblestone, sensa-tion when multiple myomas are present. Occasionally, these large myomas present as a large asymptomatic pelvic or even abdominopelvic mass. Such large leiomyomata may cause an uncommon but significant clinical problem: pressure on the ureters as they traverse the pelvic brim leading to hydroureter (dilation of the ureter) and possi-bly hydronephrosis (dilation of the renal pelvis and calyces). These conditions can also occur if fibroids lower within the pelvis grow laterally between the leaves of the broad ligament.
Another presentation is the onset
of secondary dys-menorrhea. Other
pain symptoms, although rare, may bethe result of rapid enlargement of a
leiomyoma. This can result in areas of tissue necrosis or areas of subnecrotic
vas-cular ischemia, which contribute to alteration in myome-trial response to
prostaglandins similar to the mechanism described for primary dysmenorrhea.
Occasionally, torsion of a pedunculated myoma can occur, resulting in acute
pain. Dull, intermittent, low midline cramping (labor-like) pain is the
clinical presentation when a submucous (sub-endometrial) myoma becomes
pedunculated and progres-sively prolapses through the internal os of the
cervix.
Related Topics