Chapter: Essentials of Psychiatry: Dissociative Disorders
Treatment of Dissociative Identity Disorder (Multiple Personality Disorder)
Treatment
Psychotherapy
Therapeutic Direction
It is possible to help patients with DID gain control over the
dis-sociative process underlying their symptoms in several ways. The
fundamental psychotherapeutic stance should involve meet-ing patients halfway,
a form of structured empathy in which their experience of themselves as
fragmented is acknowledged while the reality that the fundamental problem is a
failure of integration of disparate memories and aspects of the self is kept in
view. In this sense, such individuals suffer from having less than one
per-sonality rather than more than one. Therefore, the goal in therapy is to
facilitate integration of disparate elements. This can be done in a variety of
ways.
Secrets are frequently a problem with such patients, who attempt to use
the psychiatrist to reinforce a dissociative strat-egy of withholding relevant
information from certain personal-ity states. Such patients often like to
confide in the psychiatrist with the idea that the information is to be kept
from other parts of the self, for example, traumatic memories or plans for
self-destructive activities.
Clear limit setting and commitment on the part of the psy-chiatrist to
helping all portions of the patient’s personality struc-ture learn about
warded-off information are important. It is wise to clarify explicitly that the
psychiatrist will not become involved in secret collusion. Furthermore, when
important agreements are negotiated, such as commitments on the part of
patients to seek medical help before acting on a thought to harm themselves or
others, it is useful to discuss with the patients that this is an “all-points
bulletin”, requiring attention from all the relevant person-ality states. The
excuse that certain personality states were “not aware” of the agreement should
not be accepted.
Hypnosis
Hypnosis can be helpful in facilitating psychotherapy as well as
establishing the diagnosis. First of all, the simple structure of hypnotic
induction may elicit dissociative phenomena. Hypnosis can be helpful in
facilitating access to dissociated personalities. They may simply occur
spontaneously during hypnotic induc-tion. An alternative strategy is to
hypnotize the patient and use age regression to reorient to a time when a
different personality state was manifest. An instruction later to change times
back to the present usually elicits a return to the other personality state.
This then becomes a means of teaching such an individual how to control the
dissociative process.
Alternatively, entering the state of hypnosis may make it possible
simply to address and elicit different identities or per-sonality states.
Patients can be taught a simple self-hypnosis ex-ercise for this purpose. For
example, the patient can be told to count to herself or himself from one to
three. After some formal exercises such as this, it is often possible to ask
the patient to speak with a given alter personality, without the formal use of
hypnosis. Merely asking to talk with a given identity usually suf-fices after a
while.
Memory Retrieval
Because the loss of memory in DID is complex and chronic,its retrieval
is likewise a more extended and integral part of the psychotherapeutic process.
The therapy becomes an integrating experience of information sharing among
disparate personality elements. Conceptualizing DID as a chronic PTSD, the
psycho-therapeutic strategy involves a focus on working through trau-matic
memories in addition to controlling the dissociation.
Controlled access to memories greatly facilitates psycho-therapy. As
with dissociative amnesia, a variety of strategies can be employed to help
patients with DID break down amnesic bar-riers. Eliciting various identities or
personality states can facili-tate access to memories previously unavailable to
consciousness. While so-called “pseudomemories” can occur, previously
disso-ciated traumatic memories are often accurate.
Once these memories of earlier traumatic experience have been brought
into consciousness, it is crucial to help the patient work through the painful
affect, inappropriate self-blame and other reactions to these memories. It may
be useful to have pa-tients visualize the memories rather than relive them as a
means of making their intensity more manageable. It can also be useful to have
patients divide the memories, for example, picturing on one side of an
imaginary screen something an abuser did to them and on the other side how they
tried to protect themselves from the abuse.
Such techniques can help make the traumatic memories more bearable by
placing them in a broader perspective, one in which trauma victims can also
identify adaptive aspects of their response to the trauma.
This and similar approaches can help these individuals work through
traumatic memories, enabling them to bear them in consciousness and therefore
reducing the need for dissocia-tion as a means of keeping such memories and
associated painful affect out of consciousness. Although these techniques can
be helpful and often result in reduced fragmentation and integra-tion, a number
of complications can occur in the psychotherapy of these patients.
The therapeutic process can be thought of as a kind of grief work in
which information retrieved from memory is reviewed, traumatic memories are put
into perspective, and emotional ex-pression is encouraged and worked through,
thereby making it more possible to endure and disseminate the information as
widely as possible among various parts of the patient’s personal-ity structure.
Instructions to other alter personalities to “listen” while a given one is
talking and reviewing previously dissociated material can be helpful.
The Rule of Thirds
The psychotherapy of DID can be a time-consuming and emo-tionally taxing
process. The rule of thirds (Kluft, 1991; Schacter, 1995) is a helpful
guideline. Spend the first third of the psycho-therapy session assessing the
patient’s current mental state and life problems and defining a problem area
that might benefit from retrieval into conscious memory and working through.
Spend the second third of the session accessing and working through this
memory. Allow a final third for helping the patient assimilate the information,
regulate and modulate emotional responses, and discuss any responses to the
psychiatrist and plans for the im-mediate future. The psychiatrist may resist
doing this becausethe intense abreactive materials are often so compelling and
in-teresting. The patient may also resist sharing information across
personalities. Nonetheless, the psychiatrist can be helpful in im-posing
structure on often chaotic memories and identity states.
Given the intensity of the material that often emerges involving
memories of sexual and physical abuse and sudden shifts in mental state
accompanied by amnesia, the psychiatrist is called on to take a clear and
structured role in managing the psychotherapy. Appropriate limits must be set
concerning self-destructive or threatening behavior, agreements must be made
regarding physical safety and treatment compliance, and other matters must be
presented to the patient in such a way that dis-sociative ignorance is not an
acceptable explanation for failure to live up to the agreements.
Traumatic Transference
Transference applies with special meaning to patients who have been
physically and sexually abused, especially in childhood. They have experienced
individuals who are presumed to be care-takers acting instead in an
exploitative and sometimes sadistic fashion. They thus expect similar betrayal
from psychiatrists. Although their reality testing is good enough that they can
per-ceive genuine caring, they often unconsciously expect psychia-trists to
exploit them. They may experience working through of traumatic memories as a
reinflicting of the trauma, with the psychiatrist taking sadistic pleasure in
their suffering. They may expect excessive passivity on the part of the
psychiatrist, iden-tifying the psychiatrist with some uncaring family figure
who knew that abuse was occurring but did little or nothing to stop it. It is
important in managing the therapy to keep these issues in mind and make them
frequent topics of discussion. This can diffuse, if not eliminate, such
traumatic transference distortions of the therapeutic relationship.
Integration
The ultimate goal of psychotherapy is integration of these multiple ego
states. It is often the case that one or more of the personality states may
exert considerable resistance to the process of integra-tion, particularly
early in the process of therapy. Also patients may experience efforts of
integration as an attempt on the part of the therapist to “kill” personalities.
These fears must be worked through and the patient needs to understand that the
goal is to learn how to control the episodes of dissociation. This gives
patients a sense of gradually being able to control their dissociative
proc-esses in order to work through the traumatic memories. In order to enhance
mastery and control, the process of the psychotherapy must help patients
minimize rather than reinforce the content of traumatic memories, which often
involves reexperiencing a sense of helplessness in a symbolic reenactment of
the trauma.
At the same time, the dissociative defense represents an internalization
of the abusive people in the patient’s past, a kind of identification with the
aggressor, which makes the patient feel powerful rather than helpless. Setting
aside the defense also means acknowledging and bearing the helplessness of
having been victimized and working through the irrational self-blame that gave
such individuals a fantasy of control over events dur-ing which they were
helpless. Yet, difficult as it is, ultimately the goal of psychotherapy is
mastery over the dissociative process, controlled access to dissociative
states, integration of warded-off painful memories and material, and a more
integrated con-tinuum of identity, memory and consciousness. Although there
have been no controlled trials of the outcome of psychotherapy.
for this disorder, case series reports indicate a positive outcome in a
majority of cases (Kluft, 1984, 1986, 1991).
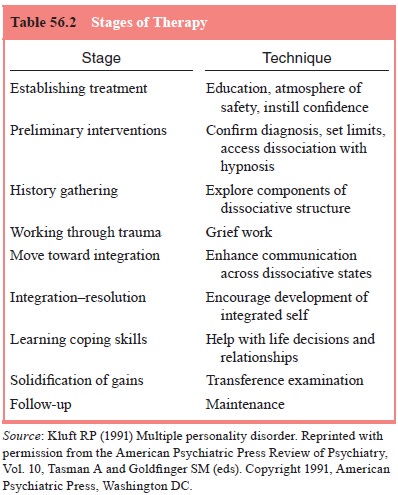
The stages of therapy are presented in Table 56.2.
Psychopharmacology
As with other dissociative disorders, there is little evidence that
psychoactive drugs are of great help in reversing dissociative symptoms
(Maldonado et al., 2000). In the
past, short-acting bar-biturates such as sodium amobarbital were used
intravenously to reverse functional amnesia, but this technique is no longer
em-ployed, largely because of poor results. Research data provide no evidence
suggesting that any medication regimen has any sig-nificant therapeutic effect
on the dissociative process manifested by DID patients. To date,
pharmacological treatment has been limited to symptom control or the management
of comorbid con-ditions (e.g., depression).
Of all available classes of psychotropic agents, antide-pressants are
the most useful class for the treatment of patients with DID. That is because
patients suffering from dissociation frequently experience comorbid dysthymic
or major depressive disorder. The newer agents – selective serotonin reuptake
inhibi-tors (SSRIs) – are particularly useful, given their high level of
effectiveness, low side-effect profile, and even lower danger in overdose,
compared with tricyclic antidepressants and monoam-ine oxidase inhibitors.
Nevertheless, medication compliance may be a problem with dissociative patients
because dissociated per-sonality states may interfere with medication taking or
may take the medication in an overdose attempt.
Benzodiazepines have mostly been used to facilitate re-call by
controlling secondary anxiety associated with retrieval of traumatic memories
(i.e., medication facilitated interviews). Nev-ertheless, despite their
short-term usefulness, CNS-depressant agents may cause sudden mental state
transitions, which may inturn increase rather than decrease amnesic barriers.
Therefore, as useful as they could be on short-term basis (i.e., acute manage-ment
of a panic attack), the long term of these agents may, in fact, contribute
rather than treat dissociative episodes.
There are several uses for anticonvulsant agents. We know that seizures
disorders have a high rate of comorbidity with DID. Thus, anticonvulsant agents
may help control the dissociation associated with epileptogenic activity. On
the other hand, anti-convulsant agents have proven to be effective in the
management of mood disorders, as well as the impulsiveness associated with
personality disorders and brain injury. Also despite their effec-tiveness,
these agents produce less amnestic side effects than the benzodiazepines and
thus may be preferred. On the other hand, the need for closer monitoring due to
potential toxicity, particu-larly in overdoses, makes their use less desirable
than the newer SSRIs.
Of all pharmacological agents available, antipsychotics may be the less
desirable. First, they are rarely useful in reduc-ing dissociative symptoms. In
fact, there have been reports of increased levels of dissociation and an
increased incidence of side effects when used in patients suffering from
dissociative disorders.
Related Topics