Chapter: Medical Physiology: Female Physiology Before Pregnancy and Female Hormones
Female Fertility
Female Fertility
Fertile Period of Each Sexual Cycle. The ovum remainsviable and capable of being fertilized after it is expelled from the ovary probably no longer than 24 hours. There-fore, sperm must be available soon after ovulation if fer-tilization is to take place. A few sperm can remain fertile in the female reproductive tract for up to 5 days. There-fore, for fertilization to take place, intercourse must occur sometime between 4 and 5 days before ovulation up to a few hours after ovulation. Thus, the period of female fertility during each month is short, about 4 to 5 days.
Rhythm Method of Contraception. One of the commonlypracticed methods of contraception is to avoid inter-course near the time of ovulation. The difficulty with this method of contraception is predicting the exact time of ovulation. Yet the interval from ovulation until the next succeeding onset of menstruation is almost always between 13 and 15 days. Therefore, if the men-strual cycle is regular, with an exact periodicity of 28 days, ovulation usually occurs within 1 day of the 14th day of the cycle. If, in contrast, the periodicity of the cycle is 40 days, ovulation usually occurs within 1 day of the 26th day of the cycle. Finally, if the periodicity of the cycle is 21 days, ovulation usually occurs within 1 day of the 7th day of the cycle. Therefore, it is usually stated that avoidance of intercourse for 4 days before the cal-culated day of ovulation and 3 days afterward prevents conception. But such a method of contraception can be used only when the periodicity of the menstrual cycle is regular.
Hormonal Suppression of Fertility—“The Pill.” It has longbeen known that administration of either estrogen or progesterone, if given in appropriate quantities during the first half of the monthly cycle, can inhibit ovulation. The reason for this is that appropriate administration of either of these hormones can prevent the preovulatory surge of LH secretion by the pituitary gland, which is essential in causing ovulation.
Why the administration of estrogen or progesterone prevents the preovulatory surge of LH secretion is not fully understood. However, experimental work has sug-gested that immediately before the surge occurs, there is probably a sudden depression of estrogen secretion by the ovarian follicles, and this might be the necessary signal that causes the subsequent feedback effect on the anterior pituitary that leads to the LH surge.The admin-istration of sex hormones (estrogens or progesterone) could prevent the initial ovarian hormonal depression that might be the initiating signal for ovulation.
The problem in devising methods for the hormonal suppression of ovulation has been in developing appro-priate combinations of estrogens and progestins that suppress ovulation but do not cause other, unwanted effects. For instance, too much of either hormone can cause abnormal menstrual bleeding patterns. However, use of certain synthetic progestins in place of proges-terone, especially the 19-norsteroids, along with small amounts of estrogens usually prevents ovulation yet allows an almost normal pattern of menstruation. Therefore, almost all “pills” used for the control of fer-tility consist of some combination of synthetic estrogens and synthetic progestins. The main reason for using syn-thetic estrogens and progestins is that the natural hor-mones are almost entirely destroyed by the liver within a short time after they are absorbed from the gastroin-testinal tract into the portal circulation. However, many of the synthetic hormones can resist this destructive propensity of the liver, thus allowing oral administration.
Two of the most commonly used synthetic estrogens are ethinyl estradiol and mestranol. Among the most commonly used progestins are norethindrone, norethyn-odrel, ethynodiol, and norgestrel. The drug is usuallybegun in the early stages of the monthly cycle and con-tinued beyond the time that ovulation would normally occur. Then the drug is stopped, allowing menstruation to occur and a new cycle to begin.
Abnormal Conditions That Cause Female Sterility. About 5 to10 per cent of women are infertile. Occasionally, no abnormality can be discovered in the female genital organs, in which case it must be assumed that the infer-tility is due to either abnormal physiological function of the genital system or abnormal genetic development of the ova themselves.
Probably by far the most common cause of female sterility is failure to ovulate. This can result from hyposecretion of gonadotropic hormones, in which case the intensity of the hormonal stimuli is simply insufficient to cause ovulation, or it can result from abnormal ovaries that do not allow ovulation. For instance, thick ovarian capsules occasionally exist on the outsides of the ovaries, making ovulation difficult.
Because of the high incidence of anovulation in sterile women, special methods are often used to determine whether ovulation occurs. These methods are based mainly on the effects of progesterone on the body, because the normal increase in progesterone secretion usually does not occur during the latter half of anovulatory cycles. In the absence of progestational effects, the cycle can be assumed to be anovulatory.
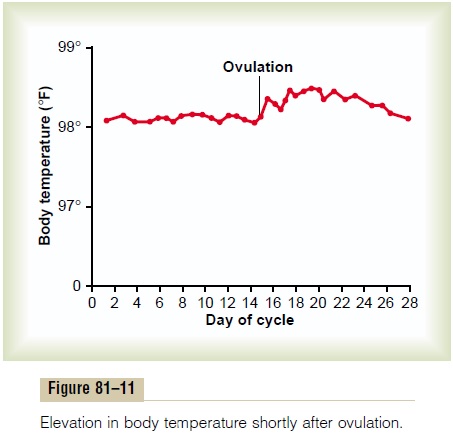
One of these tests is simply to analyze the urine for a surge in pregnanediol, the end product of progesterone metabolism, during the latter half of the sexual cycle; the lack of this substance indicates failure of ovulation. Another common test is for the woman to chart her body temperature throughout the cycle. Secretion of progesterone during the latter half of the cycle raises the body temperature about 0.5°F, with the temperature rise coming abruptly at the time of ovulation. Such a temperature chart, showing the point of ovulation, is illustrated in Figure 81–11.
Lack of ovulation caused by hyposecretion of the pituitary gonadotropic hormones can sometimes be treated by appropriately timed administration of hu-man chorionic gonadotropin, a hormone that is extracted from the human placenta. This hormone, although secreted by the placenta, has almost the same effects as LH and is therefore a pow-erful stimulator of ovulation. However, excess use of this hormone can cause ovulation from many follicles simultaneously; this results in multiple births, an effect that has caused as many as eight babies (mostly stillborn) to be born to mothers treated for infertility with this hormone.
One of the most common causes of female sterility is endometriosis, a common condition in which endome-trial tissue almost identical to that of the normal uterine endometrium grows and even menstruates in the pelvic cavity surrounding the uterus, fallopian tubes, and ovaries. Endometriosis causes fibrosis throughout the pelvis, and this fibrosis sometimes so enshrouds the ovaries that an ovum cannot be released into the abdominal cavity. Often, endometriosis occludes the fal-lopian tubes, either at the fimbriated ends or elsewhere along their extent.
Another common cause of female infertility is salp-ingitis, that is, inflammation of the fallopian tubes; thiscauses fibrosis in the tubes, thereby occluding them. In the past, such inflammation occurred mainly as a result of gonococcal infection, but with modern therapy, this is becoming a less prevalent cause of female infertility.
Still another cause of infertility is secretion of abnor-mal mucus by the uterine cervix. Ordinarily, at the time of ovulation, the hormonal environment of estrogen causes the secretion of mucus with special charac-teristics that allow rapid mobility of sperm into the uterus and actually guide the sperm up along mucous “threads.” Abnormalities of the cervix itself, such as low-grade infection or inflammation, or abnormal hor-monal stimulation of the cervix can lead to a viscous mucous plug that prevents fertilization.
Related Topics