Chapter: Medical Surgical Nursing: Perspectives in Transcultural Nursing
Culturally Competent Nursing Care
Culturally Competent Nursing Care
Culturally competent or
congruent nursing care refers to the com-plex
integration of attitudes, knowledge, and skills (including as-sessment,
decision making, judgments, critical thinking, and evaluation) that enables the
nurse to provide care in a culturally sensitive and appropriate manner. Agency
and institutional poli-cies are important to achieve culturally competent care.
Policies that promote culturally competent care establish flex-ible
regulations pertaining to visitors (number, frequency, and length of visits),
provide translation services for non–English-speaking patients, and train staff
to provide care for patients with different cultural values (Suro, 2000).
Culturally competent poli-cies also recognize the special dietary needs of
patients from se-lected cultural groups and create an environment in which the
traditional healing, spiritual, and religious practices of patients are
respected and encouraged.
Giger and Davidhizar (1999) created an assessment model to guide the nurse
in exploring cultural phenomena that might affect nursing care. They identified
communication, space, time orien-tation, social organization, environmental
control, and biologic variations as relevant phenomena (Giger & Davidhizar,
1999). This model has been used in various patient care settings to pro-vide
data essential to the provision of culturally competent care.
CROSS-CULTURAL COMMUNICATION
Establishing an
environment of culturally congruent care and re-spect begins with effective
communication, which occurs not only through words, but also through body
language and other cues, such as voice, tone, and loudness. Nurse–patient
interactions, as well as communications among members of a multicultural health
care team, are dependent on the ability to understand and be understood.
Approximately 150
different languages are spoken in the United States, with Spanish accounting
for the largest percentage after English. Obviously, nurses cannot become
fluent in all lan-guages, but certain strategies for fostering effective
cross-cultural communication are necessary when providing care for patients who
are not fluent in English. Cultural needs should be consid-ered when choosing
an interpreter; fluency in varied dialects, for instance, is beneficial (Suro,
2000). The interpreter’s voice quality, pronunciation, use of silence, use of
touch, and use of nonverbal communication should also be assessed (Giger &
Davidhizar, 1999).
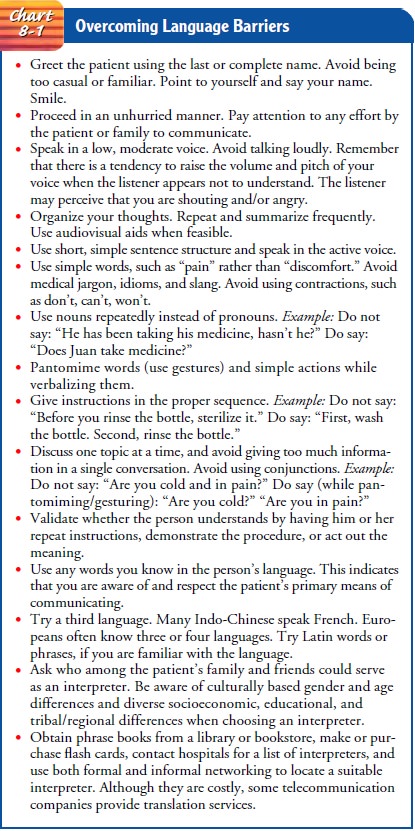
During illness, patients
of all ages tend to regress, and the regression often involves language skills.
Chart 8-1 summarizes suggested strategies for overcoming language barriers. The
nurse should also assess how well the patient and family have under-stood what
has been said. The following cues may signal lack of effective communication:
· Efforts to change the subject. This could indicate that the patient does not understand what you are saying and is at-tempting to talk about something more familiar.
·
Absence of questions. Paradoxically, this often
means that the listener is not grasping the message and therefore has
difficulty formulating questions to ask.
·
Inappropriate laughter. A self-conscious giggle may
signal poor comprehension and may be an attempt to disguise em-barrassment.
· Nonverbal cues. Although a blank expression may signal poor understanding, among some Asian Americans it may reflect a desire to avoid overt expression of emotion. Simi-larly, avoidance of eye contact may be a cultural expression of respect for the speaker; some Native Americans and Asian Americans use this gesture.
Related Topics