Chapter: Clinical Dermatology: Sebaceous and sweat gland disorders
Acne
Acne
Acne
is a disorder of the pilosebaceous apparatus characterized by comedones,
papules, pustules, cysts and scars.
Prevalence
Nearly
all teenagers have some acne (acne vulgaris). It affects the sexes equally,
starting usually between the ages of 12 and 14 years, tending to be earlier in
females. The peak age for severity in females is 16–17 and in males 17–19
years. Variants of acne are much less common.
Cause
Acne vulgaris
Many
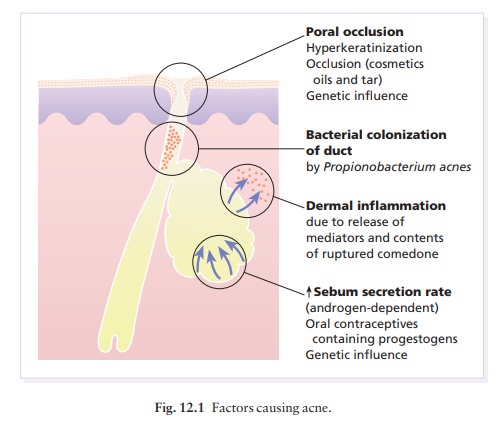
factors combine to cause acne (Fig. 12.1), characterized by chronic
inflammation around pilose-baceous follicles.
•
Sebum. Sebum excretion is increased.
However,this alone need not cause acne; patients with acro-megaly, or with
Parkinson’s disease, have high sebum excretion rates but no acne. Furthermore,
sebum excretion often remains high long after the acne has gone away.
•
Hormonal. Androgens (from the testes,
ovaries andadrenals) are the main stimulants of sebum excretion, although other
hormones (e.g. thyroid hormones and growth hormone) have minor effects too.
Those castrated before puberty never develop acne. In acne, the sebaceous
glands respond excessively to what are usually normal levels of these hormones
(increased target organ sensitivity). This may be caused by 5α-reductase activity being higher in the target sebaceous
glands than in other parts of the body. Fifty per cent of females with acne
have slightly raised free testos-terone levelsausually because of a low level
of sex hormone binding globulin rather than a high total testosteroneabut this
is still only a fraction of the concentration in males, and its relevance is
debatable.
Poral occlusion. Both genetic and environmentalfactors (e.g. some cosmetics) cause the epithelium to overgrow the follicular surface. Follicles then retain sebum that has an increased concentration of bacteria and free fatty acids. Rupture of these follicles is asso-ciated with intense inflammation and tissue damage, mediated by oxygen free radicals and enzymes such as elastase, released by white cells.
•
Bacterial. Propionibacterium acnes,
a normal skincommensal, plays a pathogenic part. It colonizes the pilosebaceous
ducts, breaks down triglycerides releas-ing free fatty acids, produces
substances chemotactic for inflammatory cells and induces the ductal epithelium
to secrete pro-inflammatory cytokines. The inflammat-ory reaction is kept going
by a type IV immune reaction to one or
more antigens in the follicle.
•
Genetic. The condition is familial in about
half ofthose with acne. There is a high concordance of the sebum excretion rate
and acne in monozygotic, but not dizygotic, twins. Further studies are required
to determine the precise mode of inheritance.
Variants of acne
•
Infantile acne may follow transplacental
stimu-lation of a child’s sebaceous glands by maternal androgens.
•
Mechanical. Excessive scrubbing, picking, or
therubbing of chin straps or a fiddle (see Fig. 12.2) can rupture occluded
follicles.

• Acne associated with virilization, including clito-romegaly, may be caused by an androgen-secreting tumour of the adrenals, ovaries or testes or, rarely, to congenital adrenal hyperplasia caused by mild 21-hydroxylase deficiency. The gene frequency for this autosomal recessive disorder is high in Ashkenazi Jews (19%), inhabitants of the former Yugoslavia (12%) and Italians (6%).
•
Acne accompanying the polycystic ovarian syndrome is
caused by modestly raised circulating androgen levels.
•
Drug-induced. Corticosteroids, androgenic
andanabolic steroids, gonadotrophins, oral contracept-ives, lithium, iodides,
bromides, antituberculosis and anticonvulsant therapy can all cause an acneiform
rash.
•
Tropical. Heat and humidity are responsible
forthis variant, which affects Caucasoids with a tendency to acne.
•
Acne cosmetica.
Presentation
Common type
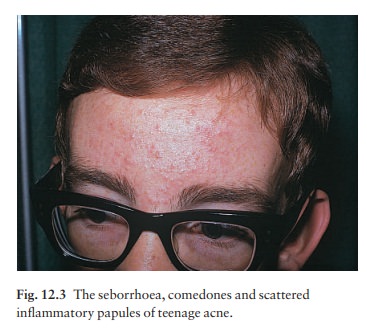
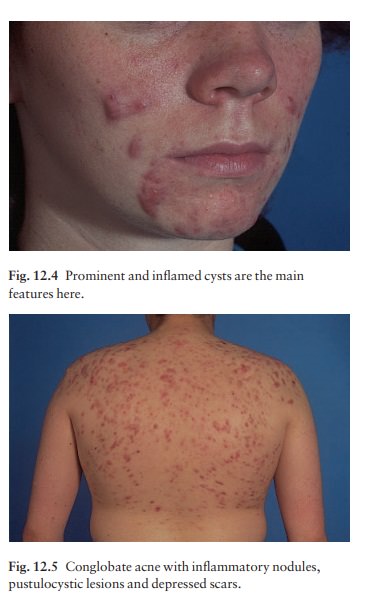
Lesions are confined to the face, shoulders, upper chest and back. Seborrhoea (a greasy skin; Fig. 12.3) is often present. Open comedones (blackheads), because of the plugging by keratin and sebum of the pilose-baceous orifice, or closed comedones (whiteheads), caused by overgrowth of the follicle openings by surrounding epithelium, are always seen. Inflammat-ory papules, nodules and cysts (Figs 12.4 and 12.5) occur, with one or two types of lesion predominating. Depressed or form of acne with all of the above features as well as abscesses or cysts with intercommunicating sinuses that contain thick serosanguinous fluid or pus. On resolution, it leaves deeply pitted or hypertrophic scars, sometimes joined by keloidal bridges. Although hyperpigmentation is usually transient, it can persist, particularly in those with an already dark skin.
Psychological
depression is common in persistent acne, which need not necessarily be severe.
Variants
Infantile.
This rare type of acne is present at, orappears soon after birth. It is more
common in males and may last up to 3 years. Its morphology is like that of
common acne (Fig. 12.6) and it may be the forerun-ner of severe acne in
adolescence

• Fulminans.
Acne fulminans is a rare variant inwhich conglobate acne is accompanied by
fever, joint pains and a high erythrocyte sedimentation rate (ESR).
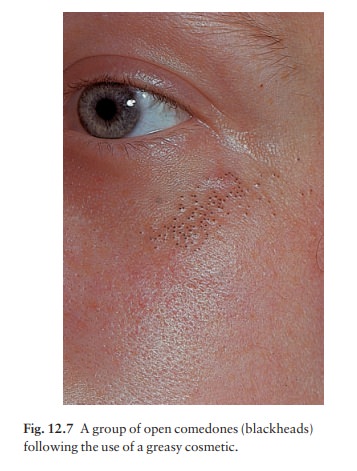
• Exogenous.
Tars, chlorinated hydrocarbons, oils,and oily cosmetics can cause or exacerbate
acne. Suspicion should be raised if the distribution is odd or if comedones
predominate (Fig. 12.7).
• Excoriated.
This is most common in young girls.Obsessional picking or rubbing leaves
discrete denuded areas.
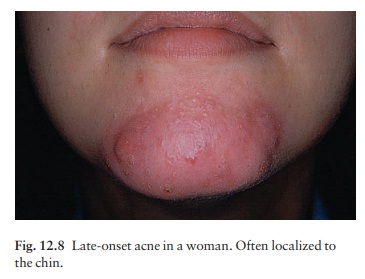
• Late
onset. This too occurs mainly in women and isoften limited to the
chin (Fig. 12.8). Nodular and cys-tic lesions predominate. It is stubborn and
persistent.
• Acne associated
with suppurative hidradenitis and perifolliculitis of scalp .
• Tropical.
This occurs mainly on the trunk and maybe conglobate.
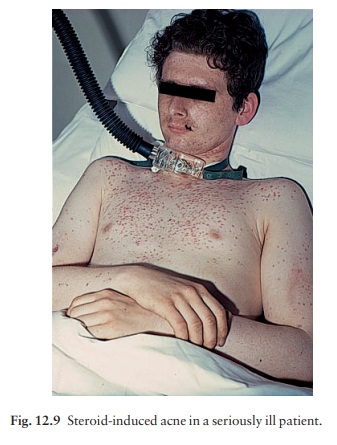
Drug-induced
(Fig. 12.9). Suspicion should be raisedwhen acne, dominated
by papulo-pustules rather than comedones, appears suddenly in a non-teenager
and coincides with the prescription of a drug known to cause acneiform lesions
. Some athletes still use anabolic steroids to enhance their performance.
• Polycystic
ovarian syndrome. Consider this in obesefemales with oligomenorrhoea or
secondary amenor-rhoea or infertility. Glucose intolerance, dyslipidaemia and
hypertension may be other features.
Congenital adrenal hyperplasia. Hyperpigmenta-tion, ambiguous genitalia, history of salt-wasting in childhood, and a Jewish background, are all clues to this rare diagnosis.
• Androgen-secreting
tumours. These cause the rapidonset of virilization (clitoromegaly,
deepening of voice, breast atrophy, male pattern balding and hirsutism) as well
as acne.
Course
Acne
vulgaris clears by the age of 23– 25 years in 90% of patients, but some 5% of
women and 1% of men still need treatment in their thirties or even forties.
Investigations
None
are usually necessary. Cultures are occasionally needed to exclude a pyogenic
infection, an anaerobic infection or Gram-negative folliculitis. Only a few
laboratories routinely culture P. acnes and test its sensitivity to
antibiotics.
Any
acne, including infantile acne, which is associ-ated with virilization, needs
investigation to exclude an androgen-secreting tumour of the adrenals, ovaries
or testes, and to rule out congenital adrenal hyper-plasia caused by
21-hydroxylase deficiency. Tests should then include the measurement of plasma
testos-terone, sex hormone-binding globulin, luteinizing hormone (LH),
follicle-stimulating hormone (FSH), dehydroepiandros-terone sulphate,
androstenedione,
17-hydroxyprogesterone,
urinary free cortisol and, depending on the results, ultrasound examination or
computed tomography scan of the ovaries and adrenals. Congenital adrenal
hyperplasia is associated with high levels of 17-hydroxyprogesterone, and
andro-gensecreting tumours with high androgen levels.
Polycystic
ovarian syndrome is characterized by modestly elevated testosterone,
androstenedione and dehydroepiandrosterone sulphate levels, a reduced sex
hormone-binding level and a LH : FSH ratio of greater than 2.5 : 1. Pelvic
ultrasound may reveal mul-tiple small ovarian cysts, although some acne
patients have ovarian cysts without biochemical evidence of the polycystic
ovarian syndrome.
Differential diagnosis
Rosacea affects older individuals; come-dones are
absent; the papules and pustules occur only on the face; and the rash has an
erythematous background. Pyogenic folliculitis can be excluded by culture.
Hidradenitis suppurativa is associated
with acne conglobata, but attacks the axillae and groin. Pseudofolliculitis barbae,
caused by ingrowing hairs, occurs on the necks of men with curly facial hair
and clears up if shaving is stopped.
Related Topics