Chapter: Medical Physiology: Somatic Sensations: II. Pain, Headache, and Thermal Sensations
Visceral Pain
Visceral Pain
In clinical diagnosis, pain from the different viscera of the abdomen and chest is one of the few criteria that can be used for diagnosing visceral inflammation, visceral infectious disease, and other visceral ailments. Often, the viscera have sensory receptors for no other modalities of sensation besides pain. Also, visceral pain differs from surface pain in several important aspects.
One of the most important differences between surface pain and visceral pain is that highly localized types of damage to the viscera seldom cause severe pain. For instance, a surgeon can cut the gut entirely in two in a patient who is awake without causing signifi-cant pain. Conversely, any stimulus that causes diffusestimulation of pain nerve endings throughout a viscuscauses pain that can be severe. For instance, ischemia caused by occluding the blood supply to a large area of gut stimulates many diffuse pain fibers at the same time and can result in extreme pain.
Causes of True Visceral Pain
Any stimulus that excites pain nerve endings in diffuse areas of the viscera can cause visceral pain. Such stimuli include ischemia of visceral tissue, chemical damage to the surfaces of the viscera, spasm of the smooth muscle of a hollow viscus, excess distention of a hollow viscus, and stretching of the connective tissue surrounding or within the viscus. Essentially all visceral pain that orig-inates in the thoracic and abdominal cavities is trans-mitted through small type C pain fibers and, therefore, can transmit only the chronic-aching-suffering type of pain.
Ischemia. Ischemia causes visceral pain in the same waythat it does in other tissues, presumably because of the formation of acidic metabolic end products or tissue-degenerative products such as bradykinin, proteolytic enzymes, or others that stimulate pain nerve endings.
Chemical Stimuli. On occasion, damaging substances leakfrom the gastrointestinal tract into the peritoneal cavity. For instance, proteolytic acidic gastric juice often leaks through a ruptured gastric or duodenal ulcer. This juice causes widespread digestion of the visceral peritoneum, thus stimulating broad areas of pain fibers. The pain is usually excruciatingly severe.
Spasm of a Hollow Viscus. Spasm of a portion of the gut,the gallbladder, a bile duct, a ureter, or any other hollow viscus can cause pain, possibly by mechanical stimula-tion of the pain nerve endings. Or the spasm might cause diminished blood flow to the muscle, combined with the muscle’s increased metabolic need for nutrients, thus causing severe pain.
Often pain from a spastic viscus occurs in the form of cramps, with the pain increasing to a high degree ofseverity and then subsiding. This process continues intermittently, once every few minutes. The intermittent cycles result from periods of contraction of smooth muscle. For instance, each time a peristaltic wave travels along an overly excitable spastic gut, a cramp occurs. The cramping type of pain frequently occurs in appen-dicitis, gastroenteritis, constipation, menstruation, par-turition, gallbladder disease, or ureteral obstruction.
Overdistention of a Hollow Viscus. Extreme overfilling of ahollow viscus also can result in pain, presumably because of overstretch of the tissues themselves. Overdistention can also collapse the blood vessels that encircle the viscus or that pass into its wall, thus perhaps promoting ischemic pain.
Insensitive Viscera. A few visceral areas are almost com-pletely insensitive to pain of any type. These include the parenchyma of the liver and the alveoli of the lungs. Yet the liver capsule is extremely sensitive to both direct trauma and stretch, and the bile ducts are also sensitive to pain. In the lungs, even though the alveoli are insen-sitive, both the bronchi and the parietal pleura are very sensitive to pain.
“Parietal Pain” Caused by Visceral Disease
When a disease affects a viscus, the disease process often spreads to the parietal peritoneum, pleura, or pericardium. These parietal surfaces, like the skin, are supplied with extensive pain innervation from the peripheral spinal nerves. Therefore, pain from the pari-etal wall overlying a viscus is frequently sharp. An example can emphasize the difference between this pain and true visceral pain: a knife incision through the parietal peritoneum is very painful, whereas a similarcut through the visceral peritoneum or through a gut wall is not very painful, if painful at all.
Localization of Visceral Pain— “Visceral” and the “Parietal” Pain Transmission Pathways
Pain from the different viscera is frequently difficult to localize, for a number of reasons. First, the patient’s brain does not know from firsthand experience that the different internal organs exist; therefore, any pain that originates internally can be localized only generally. Second, sensations from the abdomen and thorax are transmitted through two pathways to the central nervous system—the true visceral pathway and the pari-etal pathway. True visceral pain is transmitted via painsensory fibers within the autonomic nerve bundles, and the sensations are referred to surface areas of the body often far from the painful organ. Conversely, parietal sensations are conducteddirectly into local spinal nerves from the parietal peritoneum, pleura, or peri-cardium, and these sensations are usually localizeddirectly over the painful area.
Localization of Referred Pain Transmitted via Visceral Pathways.
When visceral pain is referred to the surface of the body, the person generally localizes it in the dermatomal segment from which the visceral organ originated in the embryo, not necessarily where the visceral organ now lies. For instance, the heart originated in the neck and upper thorax, so that the heart’s visceral pain fibers pass upward along the sympathetic sensory nerves and enter the spinal cord between segments C-3 and T-5. There-fore, as shown in Figure 48–6, pain from the heart is referred to the side of the neck, over the shoulder, over the pectoral muscles, down the arm, and into the sub-sternal area of the upper chest. These are the areas of the body surface that send their own somatosensory nerve fibers into the C-3 to T-5 cord segments. Most fre-quently, the pain is on the left side rather than on the right because the left side of the heart is much more fre-quently involved in coronary disease than the right.
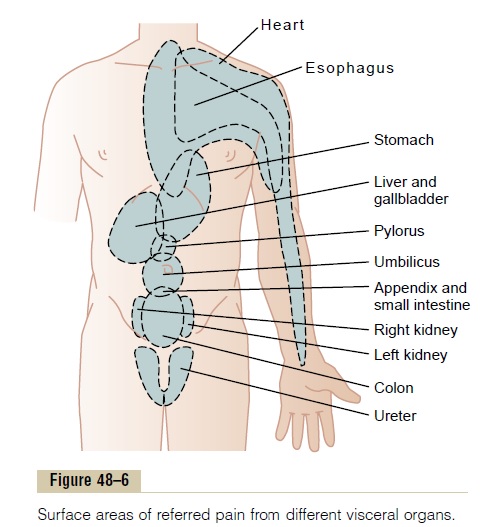
The stomach originated approximately from the seventh to ninth thoracic segments of the embryo. Therefore, stomach pain is referred to the anterior epi-gastrium above the umbilicus, which is the surface area of the body subserved by the seventh through ninth tho-racic segments. Figure 48–6 shows several other surface areas to which visceral pain is referred from other organs, representing in general the areas in the embryo from which the respective organs originated.
Parietal Pathway for Transmission of Abdominal and Thoracic Pain. Pain from the viscera is frequently localized to twosurface areas of the body at the same time because of
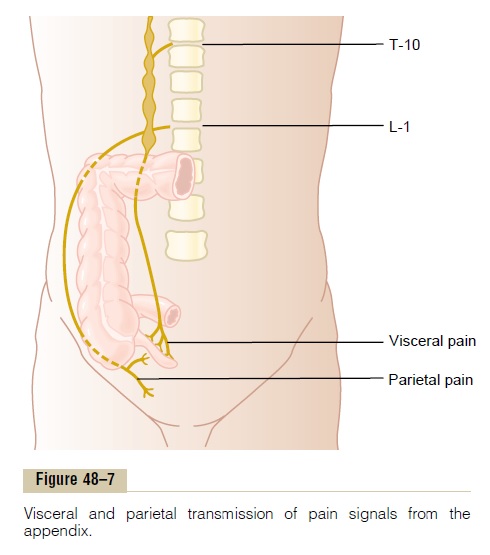
the dual transmission of pain through the referred vis-ceral pathway and the direct parietal pathway. Thus, Figure 48–7 shows dual transmission from an inflamed appendix. Pain impulses pass first from the appendix through visceral pain fibers located within sympathetic nerve bundles, and then into the spinal cord at about T-10 or T-11; this pain is referred to an area around the umbilicus and is of the aching, cramping type. Pain impulses also often originate in the parietal peritoneum where the inflamed appendix touches or is adherent to the abdominal wall. These cause pain of the sharp type directly over the irritated peritoneum in the right lower quadrant of the abdomen.
Related Topics