Chapter: Pathology: Cardiac Pathology
Valvular Heart Disease
VALVULAR HEART DISEASE
Degenerative calcific aortic valve
stenosis is a common valvular abnormality char-acterized by age
-related dystrophic calcification, degeneration, and stenosis of the aortic
valve. It is common in congenital bicuspid aortic valves. It can lead to
concen-tric left ventricular hypertrophy (LVH) and congestive heart failure
with increased risk of sudden death. The calcifications are on the outflow side
of the cusps. Treat-ment is aortic valve replacement.
Mitral valve prolapse has
enlarged, floppy mitral valve leaflets that prolapse intothe left atrium and
microscopically show myxomatous degeneration. The condi-tion affects
individuals with Marfan syndrome. Patients are asymptomatic and a mid-systolic
click can be heard on auscultation. Complications include infectious
endocarditis and septic emboli, rupture of chordae tendineae with resulting
mitral insufficiency, and rarely sudden death.
Rheumatic valvular heart disease/acute rheumatic fever
Rheumatic
fever is a systemic recurrent inflammatory disease, triggered by a
pha-ryngeal infection with Group A β-hemolytic streptococci.
In genetically susceptible individuals, the infection results in production of
antibodies that cross-react with cardiac antigens (type II hypersensitivity
reaction). Rheumatic fever affects children (ages 5–15 years), and there is a
decreasing incidence in the United States. Symptoms occur 2–3 weeks after a
pharyngeal infection; laboratory studies show elevated anti-streptolysin O
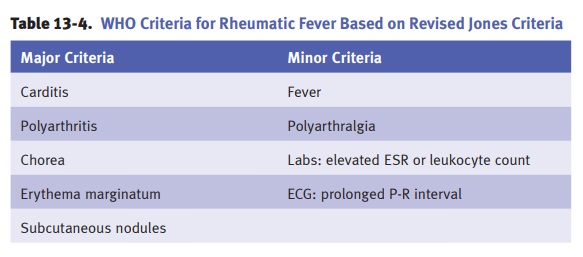
(ASO) titers. The Jones criteria are illustrated below.
Diagnosis
of rheumatic fever requires 2 major OR
1 major and 2 minor criteria, plus a
preceding group A strep infection.
·
Acute rheumatic heart disease affects
myocardium, endocardium, and peri-cardium. The myocardium can develop
myocarditis, whose most distinctive feature is the Aschoff body, in which
fibrinoid necrosis is surrounded by macrophages (Anitschkow cells),
lymphocytes, and plasma cells. Fibrinous pericarditis may be present.
Endocarditis may be a prominent feature that typically involves mitral and
aortic valves (forming fibrin vegetations along the lines of closure) and may
also cause left atrial endocardial thickening (MacCallum plaques).
·
Chronic rheumatic heart disease is
characterized by mitral and aortic valvularfibrosis, characterized by valve
thickening and calcification; fusion of the valve commissures; and damaged
chordae tendineae (short, thickened, and fused). Complications can include
mitral stenosis and/or regurgitation, aortic steno-sis and/or regurgitation,
congestive heart failure, and infective endocarditis.
Infectious bacterial endocarditis refers
to bacterial infection of the cardiac valves,characterized by vegetations on
the valve leaflets. Risk factors include rheumatic heart disease, mitral valve
prolapse, bicuspid aortic valve, degenerative calcific aor-tic stenosis,
congenital heart disease, artificial valves, indwelling catheters, dental
procedures, immunosuppression, and intravenous drug use.
·
Acute endocarditis is
typically due to ahigh virulence organismthat
can colo-nize a normal valve, such as Staphylococcus
aureus. Acute endocarditis pro-duces large destructive vegetations (fibrin,
platelets, bacteria, and neutrophils). The prognosis is poor, with mortality of
10–40%.
·
Subacute endocarditis is
typically due to a low virulence organism, such asStreptococcus group viridians, which usually colonizes a previously
damagedvalve. The disease course is typically indolent with <10% mortality.
Clinically,
endocarditis presents with fever, chills, weight loss, and cardiac murmur.
Embolic phenomena may occur, and may affect systemic organs; retina (Roth
spots); and distal extremities (Osler nodes [painful, red subcutaneous nodules
on the fin-gers and toes], Janeway lesions [painless, red lesions on the palms
and soles], and splinter fingernail hemorrhages). Diagnosis is by serial blood
cultures. Complica-tions include septic emboli, valve damage resulting in
insufficiency and congestive heart failure, myocardial abscess, and dehiscence
of an artificial heart valve.
Marantic
endocarditis (nonbacterial thrombotic endocarditis [NBTE]) is
character-ized by small, sterile vegetations along the valve leaflet line of
closure in patients with a debilitating disease. The major complications are
embolism and secondary infection of the vegetations.
Related Topics