Chapter: Basic Radiology : Scope of Diagnostic Imaging
Ultrasonography
ULTRASONOGRAPHY
Diagnostic ultrasound is a
noninvasive imaging technique that uses high-frequency sound waves greater than
20 kilo-hertz (kHz). A device known as a transducer
is used to emit and to receive sound waves from various tissues in the body.
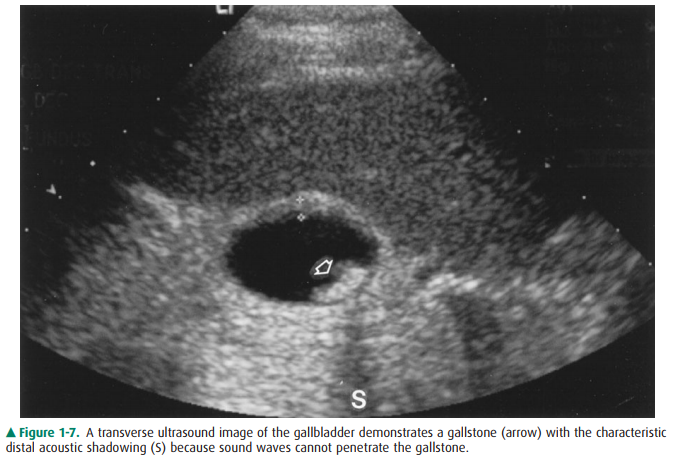
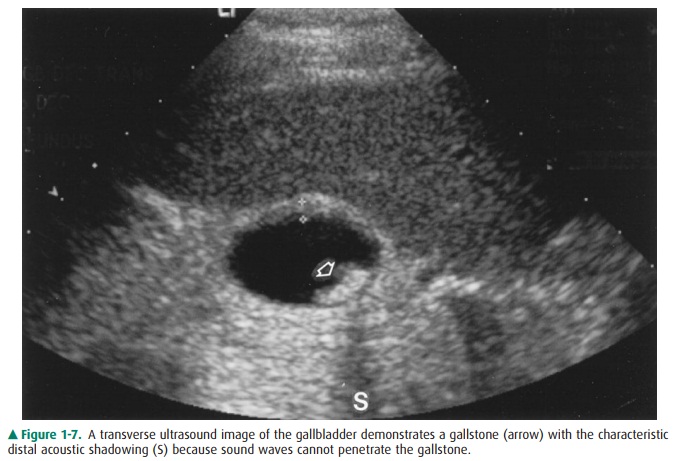
Figure 1-7. A transverse ultrasound image of the gallbladder demonstrates a
gallstone (arrow) with the characteristic distal acoustic shadowing (S) because
sound waves cannot penetrate the gallstone.
The transducer is placed against
the patient’s skin with a thin layer of coupling gel. This gel displaces the
air that would oth-erwise reflect virtually the entire incident ultrasound
beam. As sound travels into the patient, wave fronts spread out, di-minishing
the overall beam intensity. Beam attenuation also occurs secondary to partial
tissue absorption with associated heat conversion. At tissue interfaces, the
beam is partially re-flected and transmitted. The reflected sound waves, or
echoes, travel back to the transducer and are converted into electric signals
and amplified. The amplitude of the returning wave partially depends on the
degree of beam absorption. A shade of gray is then assigned to each amplitude,
with strong echoes being typically assigned a shade near the white end of the
spectrum, and weak echoes assigned a shade near the black end of the spectrum.
In addition, the depth of the reflecting tissue can be calculated from the
known total beam travel time and the average sound velocity in human tissue
(1,540 m/s). Limitations of this modality are primarily operator-dependent in
nature. Additional limitations include variable visualiza-tion of midline
abdominal organs (pancreas) and vasculature when obscured by overlying bowel gas,
as well as inability of sound waves to penetrate gas or bone.
There are many common
applications of ultrasonogra-phy, including imaging of the abdomen (liver,
gallbladder, pancreas, kidneys) (Figure 1-7), pelvis (female reproductive
organs), fetus (routine fetal surveys for detection of anom-alies), vascular
system (aneurysms, arterial-venous commu-nications, deep venous thrombosis),
testicles (tumor, torsion, infection), breasts, pediatric brain (hemorrhage,
congenital malformations), and chest (size and location of pleural fluid
collections). In addition, ultrasound-guided interventions are routinely used
to facilitate lesion biopsy, abscess drainage, and radiofrequency ablation.
Doppler ultrasound is used
primarily to evaluate vascular flow by detecting frequency shifts in the
reflected beam, uti-lizing a principle termed the Doppler effect. This effect occurs when a sound emitter or
reflector is moving relative to the stationary receiver of sound. Objects
moving toward the de-tector appear to have a higher frequency and shorter
wave-length, whereas objects moving away from the detector appear to have a
lower frequency and longer wavelength. If the ultrasound beam strikes a
reflector moving toward it, the reflected sound will have a higher frequency
than the original beam. Alternatively, if the ultrasound beam strikes a
reflectormoving away from it, the reflected sound will have a lower fre-quency
than the original beam. The Doppler shift is the fre-quency difference between
the original beam frequency and the reflected beam frequency. Frequency
differences are used to calculate the corresponding flow velocities, from which
a Doppler waveform, or tracing, can be generated. This tracing depicts the
relationship between velocity and time and is unique to the flow pattern within
the vessel. Color flow Doppler assigns colors (blue and red) to structures
according to their motion toward or away from transducers. This information can
be superimposed on a gray-scale image. Endoluminal sonography uses a high-frequency
catheter-based transducer (9 to 20 megahertz [MHz]) to image structures beyond
the lumen of the hollow viscus. It is accurate in local staging of cancer and
in detecting small lesions that may not be visualized with other imaging
modalities. Limitations for optimal evalu-ation include inability to precisely
position the transducer within an area of interest that may restrict full
entry.
Diverse applications of
ultrasonography are presented as follows. Gastrointestinal (GI) applications of
endoluminal sonography include quantification of the size and wall thick-ness
of esophageal carcinoma or to detect and characterize esophageal varices.
Transrectal ultrasound is performed to evaluate the prostate gland.
Transesophageal echocardiogra-phy is used for evaluating cardiovascular
abnormalities. Gen-itourinary (GU) applications include guidance of collagen
injections, examination of the severity and length of ureteral strictures,
diagnosis of upper-tract neoplasms and urethral diverticula, identification of
submucosal calculi, and visuali-zation of crossing vessels prior to
endopyelotomy. Evaluation of the uterus, adnexa, and fetus can be conducted
using a transvaginal probe in the presence of an empty bladder.
Sonohysterography, an ultrasound-guided procedure, re-quires instillation of a
sterile saline solution into the uterine cavity following cannulation for
evaluation of endometrial masses or other abnormalities. More recently,
intravascular application of sonography has been promising for quantitat-ing
the degree of arterial stenosis, and for monitoring the therapeutic effects of
angioplasty in both peripheral and coronary arteries. Intravascular ultrasound
(IVUS) has been applied to modeling plaque morphology, blood flow, and the
geometry of the vessel lumen. Three-dimensional ultrasound (3D-US) has been
developed with advancements in com-puter processing power and has rapidly
achieved widespread use for some clinical applications, including the
evaluation of normal embryonic and/or fetal development, as well as car-diac
morphology in specific congenital anomalies.
Related Topics