Chapter: Clinical Dermatology: Other genetic disorders
Tuberous sclerosis
Tuberous
sclerosis
This
uncommon condition, with a prevalence of about 1 in 12 000 in children under 10
years, is also inherited as an autosomal dominant trait, with variable
expressivity even within the same family. As fertility is reduced, transmission
through more than two generations is rare.
Cause
Mutations at two different loci can, independently, cause clinically identical tuberous sclerosis. The prod-uct of one gene (TSC1), lying at 9q34, is hamartin; that encoded by the other gene (TSC2) is tuberin. Both are associated in vivo, and probably act in the same biological pathways as tumour suppressors. TSC1 gene mutations are responsible for a minorityof cases and are under-represented in sporadic cases
Clinical features
The
skin changes include the following.
ŌĆó
Small oval white patches (ŌĆśash leaf
maculesŌĆÖ) occurin 80% of those affected. These are important as they may be the
only manifestation at birth.
ŌĆó
Adenoma sebaceum occur in
85% of thoseaffected. They develop at puberty as pink or yellowish acne-like
papules on the face, often around the nose (Fig. 21.4).

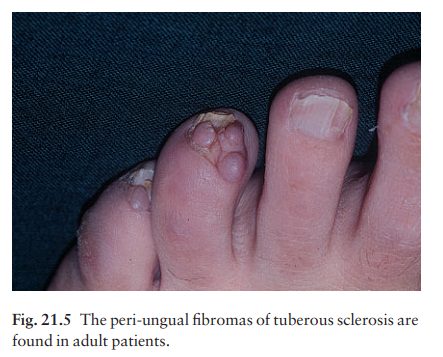
ŌĆó
Peri-ungual fibromas occur in
50% of patients.These develop in adult life as small pink sausage-like lesions
emerging from the nail folds (Fig. 21.5).
ŌĆó
Connective tissue naevi (ŌĆśshagreen
patchesŌĆÖ) are seenin 40% of patients. Cobblestone, somewhat yellow plaques
often arise in the skin over the base of the spine.
Other
features may include:
ŌĆó
epilepsy (in 75% of patients);
ŌĆó
mental retardation (in 50% of
patients);
ŌĆó
ocular signs, including retinal
phakomas and pig-mentary abnormalities (in 50% of patients);
hyperplastic gums;
ŌĆó
gliomas along the lateral walls of
the lateral vent-ricles (80% of cases) and calcification of the basal ganglia;
and
ŌĆó
renal and heart tumours.
Diagnosis and differential diagnosis
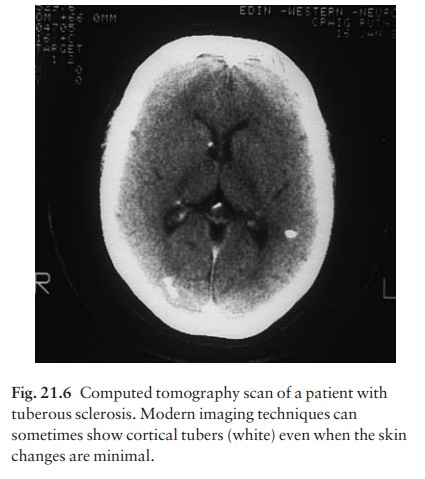
Any
baby with unexplained epilepsy should be examined with a WoodŌĆÖs light to look for ash leaf macules. Skull X-rays
and computer assisted tomography scans (Fig. 21.6) help to exclude involve-ment
of the central nervous system and kidneys. The lesions of adenoma sebaceum (a
misnomer, as histologically they are angiofibromas) may be mis-taken for acne.
Management
Affected
families need genetic counselling. Apparently unaffected parents with an
affected child will wish to know the chances of further children being
affected. Before concluding that an affected child is the result of a new
mutation, the parents should be examined with a WoodŌĆÖs light and by an
ophthalmologist to help exclude the possibility of genetic transmission from a
subtly affected parent. As the gene defects become established, prenatal
screening of DNA should indic-ate those at risk.
Adenoma
sebaceum improves cosmetically after electrodessication, dermabrasion or
destruction by laser but tends to recur.
Related Topics