Chapter: Obstetrics and Gynecology: Ectopic Pregnancy and Abortion
Tubal Ectopic Pregnancy: Management
MANAGEMENT
Management may be either surgical
or medical, depending on a variety of factors. Surgery may be minimal or
extensive, depending on the gestational age of the pregnancy and other factors.
Due to the inherent risks of each, medical therapy is preferred over surgery in
appropriate patients.
Medical Management Methotrexateis the medical treat-ment usually used as an alternative to
surgical therapy. Methotrexate is a folic acid antagonist that competi-tively
inhibits the binding of dihydrofolic acid to dihydro-folate reductase, which in
turn reduces the amount of active intracellular metabolite, folinic acid.
The best candidate for medical
therapy is the woman who is asymptomatic, motivated, and who has resources to
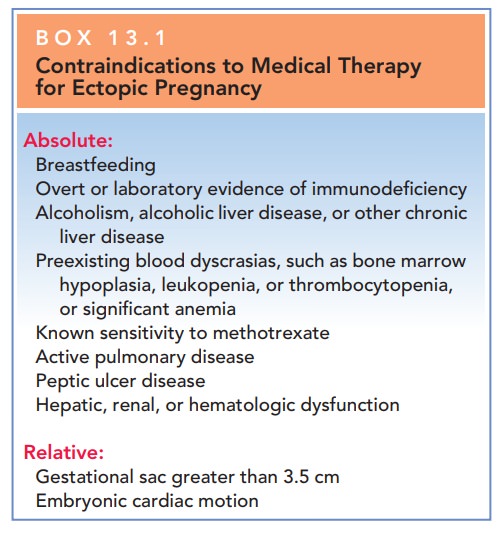
be compliant with follow-up. Relative and absolute contraindications for
medical management are listed in Box 13.1.
Factors that can be assessed in
predicting the success of medical therapy include initial β-hCG level, size of ec-topic
pregnancy as determined by TVS, and presence or absence of fetal cardiac
activity. The initial serum β-hCG
level is the single best prognostic indicator of treatment success in women
given single-dose methotrexate. An ini-tial serum value <5000 IU/L is
associated with a success rate of 92%, whereas an initial concentration
>15,000 IU/L has a success rates of 68%. Although there are few data
concerning the effect of ectopic pregnancy size on success rates with
methotrexate, many early trials used “large size” as an exclusion criterion.
Success rates with single-dose methotrexate were 93% in cases with ectopic
masses <3.5 cm. Cardiac activity and size greater than 3.5 cm are considered
relative contraindications to medical manage-ment because these findings are
associated with a lower success rate.
The most common side effects of
methotrexate in-clude nausea, vomiting, diarrhea, gastric distress, dizziness,
and stomatitis. Intramuscular methotrexate given as a single dose has been the
most widely used medical treatment of ectopic pregnancy. Close monitoring is
imperative. A serum β-hCG
level is determined before administering methotrexate and is repeated on days 4
and 7 following injection. Levels may continue to rise until day 4. Compar-ison
is then made between the day 4 and the day 7 serum values. If there is a
decline by 15% or more, weekly serum β-hCG levels are measured until they are
undetectable. Ifthe β-hCG
level does not decline, the patient may require either surgery or a second dose
of methotrexate if no con-traindications exist. If there is an adequate
treatment re-sponse, hcG determinations are reduced to once a week. An
additional dose of methotrexate may be given if β-hCG levels plateau or increase
in 7 days. Surgical intervention may be required for patients who do not
respond to med-ical therapy.
During the first few days
following methotrexate administration, up to half of women experience
abdom-inal pain that can be controlled with nonsteroidal anti-inflammatory
drugs. This pain presumably results from tubal distention caused by tubal
abortion or hematoma formation or both.
Surgical Management
Women who are hemodynami-cally stable
and in whom there is a small tubal diameter, no fetal cardiac activity, and
serum β-hCG concentrations <5000 IU/L have similar outcomes with
medical or surgi-cal management. Conservative surgical techniques have been
developed that maximize preservation of the fallopian tube. If removal is done
through the laparoscope, definitive diagnosis and treatment can be accomplished
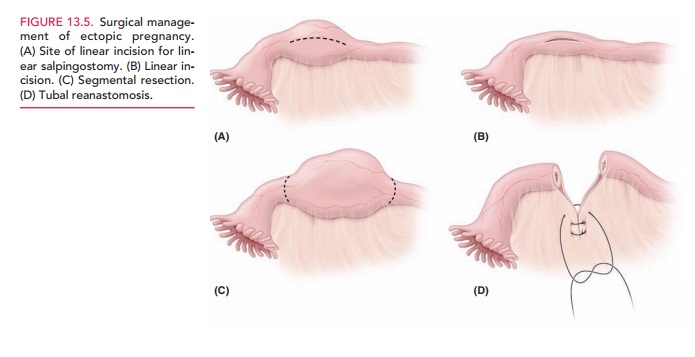
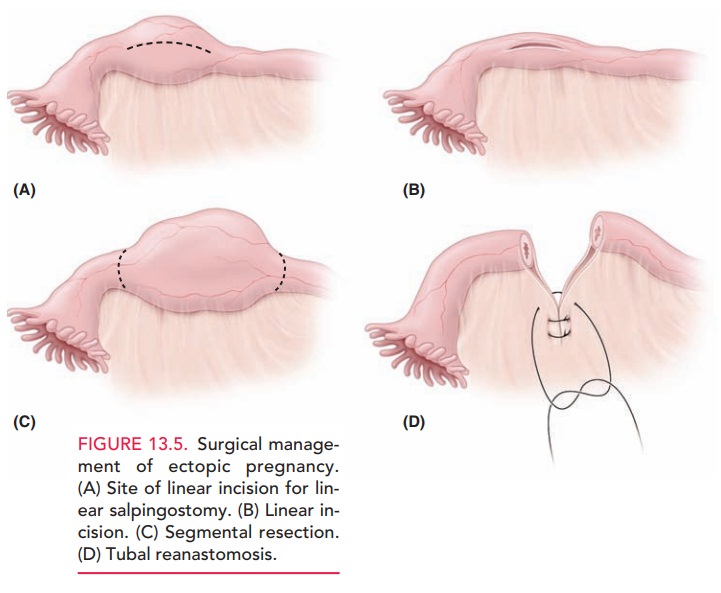
at the same operation with minimal morbidity, cost, and hospitaliza-tion. In a linear salpingostomy, the surgeon makes
an in-cision on the fallopian tube over the site of implantation, removes the
pregnancy, and allows the incision to heal by secondary intention. A segmental resection is the removal of a
portion of the affected tube (Fig. 13.5). Salpingectomy
is removal of the entire tube, a procedure reserved for those cases in which
little or no normal tube remains.
When conservative surgery or
nonsurgical treatment is used, the patient must be followed posttherapy with
serial quantitative β-hCG
levels to monitor regression of the pregnancy. Subsequent surgery or
methotrexate ther-apy is needed if trophoblastic function persists as
evi-denced by persistent or rising levels of hCG. Rh-negative mothers with
ectopic pregnancy should receive Rh
im-mune globulin to prevent Rh sensitization.
Related Topics