Chapter: Surgical Pathology Dissection : The Endocrine System
Thyroid : Surgical Pathology Dissection
Thyroid
Thyroidectomies
One
major task of the surgical pathologist evaluating a thyroid specimen is to
identify the infrequent thyroid neoplasm from among the vast majority of
harmless thyroid nodules—an effort that is shared with the cytopathologist,
endocrinologist, and surgeon. Thorough inspection and appropriate sampling of
the thyroid is central to the diagnosis and subsequent treatment of thyroid
lesions.
The
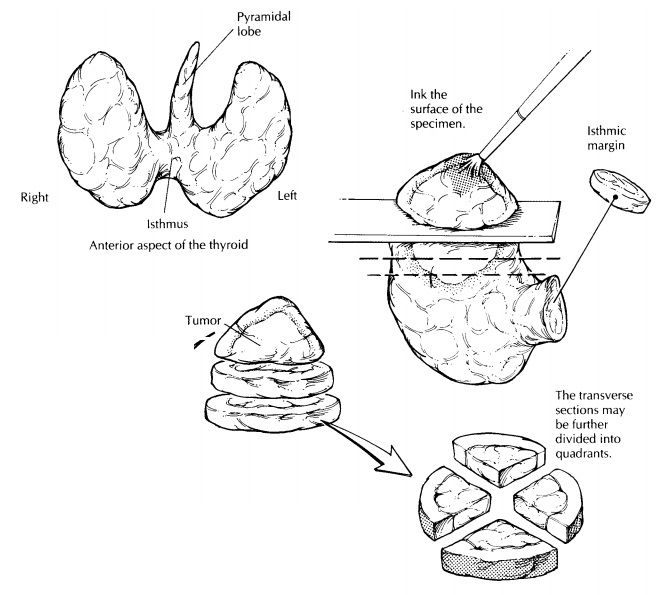
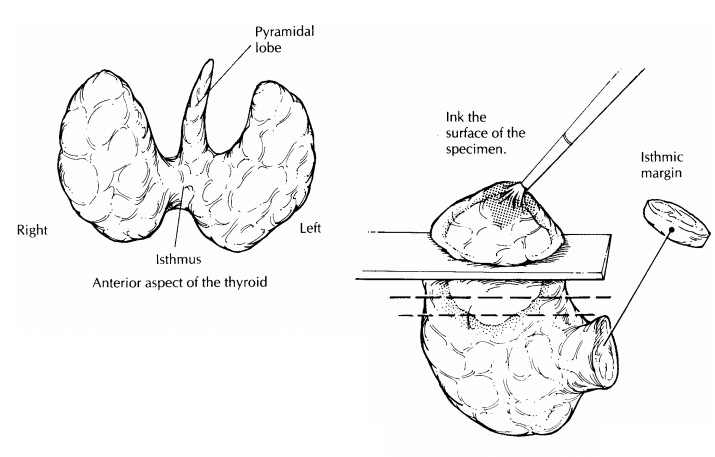
thyroid gland has a relatively simple anatomy. As illustrated, its shape
resembles that of a butterfly with open wings: two expanded lateral lobes are
bridged at the midline by the isthmus. In some specimens, a small triangular
midline lobe (i.e., the pyramidal lobe) is also present. When present, the
pyramidal lobe extends superiorly from the isthmus. The two most common
resections of the thyroid are total thyroidectomy, in which the entire gland is
removed intact, and hemithyroidectomy, in which a single lobe is removed by an
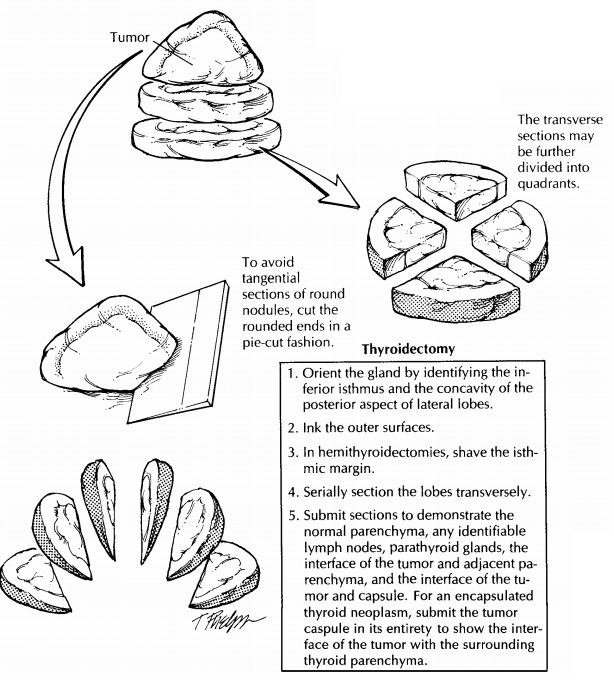
incision through the isthmus. Orientation of these specimens is seldom
problematic. The isthmus can be used to
identify the inferior and medial aspects of the gland, and the posterior
surfaces of the lateral lobes have a concave shape caused by the trachea.
Once the
specimen has been oriented, it should be weighed and measured. Describe its
shape, contours, and symmetry. Be sure to note the presence and appearance of
any extrathyroidal tissues. In particular, inspect the posterior aspect of the
specimen for parathyroid glands and lymph nodes, and inspect the anterior
aspect for fragments of adherent skeletal muscle. Palpate the specimen to assess the consistency
of the thyroid and to localize any focal lesions before cutting the specimen.
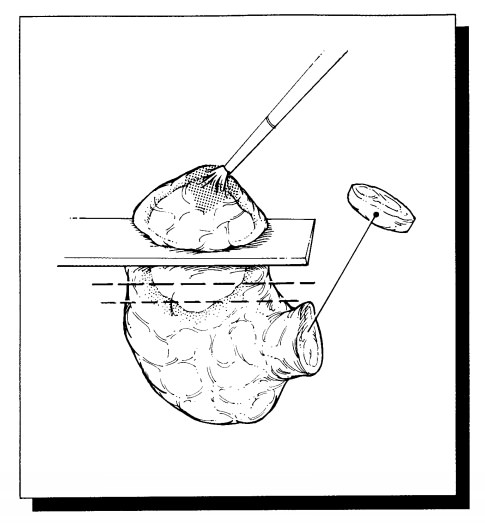
Paint
the outer surfaces of the thyroid with ink; and in the case of
hemithyroidectomy, remove the isthmic margin as a thin shave section. Although
the specimen can be serially sectioned in either the coronal, sagittal, or
transverse plane, the relationship of a focal lesion to the thyroid capsule is
often best demonstrated by cutting perpendicular to the long axis of each
individual lobe. Once the thyroid is sectioned, sequentially lay out the
individual slices in such a way as to maintain the proper orientation of the
specimen.
Carefully
inspect the cut surfaces of the specimen. Assess whether the thyroid is
diffusely or focally abnormal. For diffuse lesions, ask yourself the following
questions: Is the gland symmetrically or asymmetrically involved? Is the lesion
confined to the thyroid, or does it extend beyond the capsule of the thyroid
into the surrounding soft tissues? Is the lesion cystic or solid, soft or hard,
well demarcated or poorly defined? If an isolated lesion is identified, record
its size and location, and determine if it is surrounded by a capsule. Keep in
mind that the presence of a discrete nodule does not exclude the presence of
additional lesions. Always look for multifocal lesions. Gentle palpation of
each slice will sometimes reveal small but firm carcinomas that are not
apparent simply by looking at the cut surface.
Imprints of the tumor allow quick and easy evaluation of its cytologic features and will nicely supplement the histologic findings of a frozen section. Simply touch the surface of a glass slide to the cut surface of the tumor, or smear a small piece of the tumor between two slides, and immediately fix the slides in 95% alcohol. These slides can be used for Diff-Quik or hematoxylin and eosin staining.
Sections
for histology should be taken to dem-onstrate the following: (1) all components
of a lesion (e.g., solid areas and cystic areas); (2) the interface of the
tumor (and its surrounding cap-sule) with the adjacent non-neoplastic thyroid
parenchyma; (3) the relationship of the tumor to the thyroid capsule and
extrathyroidal soft tis-sues; and (4) the presence of parathyroids, lymph
nodes, and normal-appearing thyroid paren-chyma (one or two sections from each
lobe). Since the histologic evaluation will be hampered if the tissue blocks
are thick and bulky, you may want to consider fixing the slices in formalin
until they are firm enough to section thinly. Although these general guidelines
should direct the sam-pling of any thyroid lesions, two frequently asked
questions deserve special consideration:
How many sections do I need to submit to avoid
sampling error? This question often arises in casesof multinodular goiters and
encapsulated nod-ules. In multinodular goiters, the thyroid is often massively
enlarged, and its cut surface may show numerous nodules, hemorrhage,
calcification, scarring, and even necrosis. In these instances, try to avoid
the common error of submitting too many sections. Instead, document the finding
with a photograph and a detailed gross descrip-tion. Sampling a multinodular
goiter should be limited to one or two sections selectively taken from the
periphery of each nodule (up to five nodules per lobe). Conversely, the more
common error when sampling encapsulated nodules is to submit too few sections.
Your primary task in sampling these lesions is to make sure that areas of
transcapsular or vascular invasion are not missed. Since these areas usually
cannot be seen by the naked eye, they can easily be missed unless the
peripheral portion of the nodule is extensively sampled. The more capsule
sampled, the greater chance of finding invasive foci. Therefore, the
tumor–capsule–thyroid interface of any encapsu-lated nodule should be submitted
in its entirety for histologic evaluation.
Similarly,
thyroids removed from patients with one of the multiple endocrine neoplasia
(MEN) syndromes should be extensively sampled for histology. Many pathology
laboratories are beginning to receive thyroids prophylactically removed from
young patients with germline mutations of the ret proto-oncogene. Even thoughthese glands may appear grossly
normal, each lobe should be blocked and submitted in its entirety in an effort
to detect C-cell hyperplasia and small medullary carcinomas. In your gross
report, note those sections taken from the middle third of each lobe, as this
area is where C-cell hyperplasia and small medullary carcinomas are most likely
to be detected.![]()
How can I avoid tangential sections of a round
nodule? Tangential sections through a roundnodule may give the artifactual
microscopic im-pression that the tumor infiltrates the capsule. Whereas
tangential sectioning is usually not a problem at the equator of a nodule where
the knife easily passes perpendicular to the tumor capsule, it becomes
increasingly difficult to avoid as one approaches the rounded ends of the
nodule while bread-loafing the specimen. One method to minimize tangential
sectioning is to cut these rounded ends like a pie rather than a loaf of bread.18
Decapitate the rounded ends from the tumor nodule, place the flat surface of
each end on the cutting board, and then, as illustrated, direct each cut
perpendicular to the tumor capsule as though you were dividing a pie into equal
pieces.
Regional
neck lymph nodes are usually removed separately by the surgeon and submitted as
sepa-rate specimens. These should be anatomically ori-ented, and each level
should be carefully dissected . Each lymph node identified should be submitted
for histologic evaluation.
Important Issues to Address in Your Surgical Pathology Report on Thyroidectomies
1.
What procedure was performed, and what
structures/organs are present?
2.
What is the size of the lesion, and where is it
located? Is the tumor multifocal? If so, record the number of tumors and the
size of each.
3.
What are the histologic type and grade of the
tumor (e.g., follicular, papillary, medullary, anaplastic)?
4.
For encapsulated neoplasms, does the tumor
infiltrate its surrounding capsule?
5.
Is vascular invasion present?
6.
Is the lesion confined to the thyroid, or does
it extend beyond the thyroid capsule into the extrathyroidal soft tissues?
7.
Are any abnormalities present in the non-neoplastic
thyroid tissue (e.g., nodular hyper-plasia, thyroiditis, C-cell hyperplasia)?
8.
Is evidence of metastatic disease present?
Record the number of lymph nodes with metas-tases and the total number of lymph
nodes ex-amined. If present, note the presence of tumor extension into the
extranodal fat.
9.
If identified, note the presence and number of
parathyroid glands. Whenever possible, the location of the gland(s) should be
spec-ified.
Related Topics