Chapter: Obstetrics and Gynecology: The Woman’s Health Examination
Speculum Examination
SPECULUM EXAMINATION
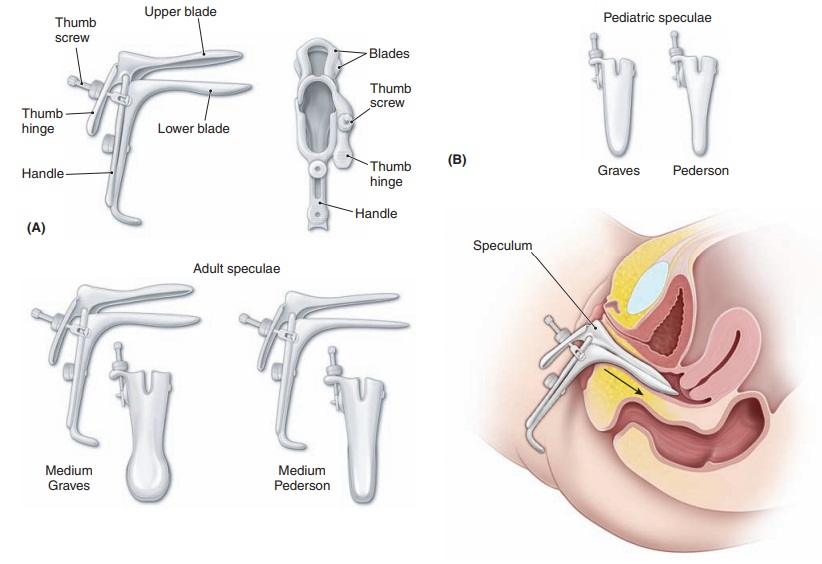
The next step is the speculum examination.The parts of thespeculum are shown in Figure 1.6. There are two types of specula in common use for the examination of adults. The Pederson speculum has flat and narrow blades that barelycurve on the sides. The Pederson speculum works well for most nulliparous women and for postmenopausal women
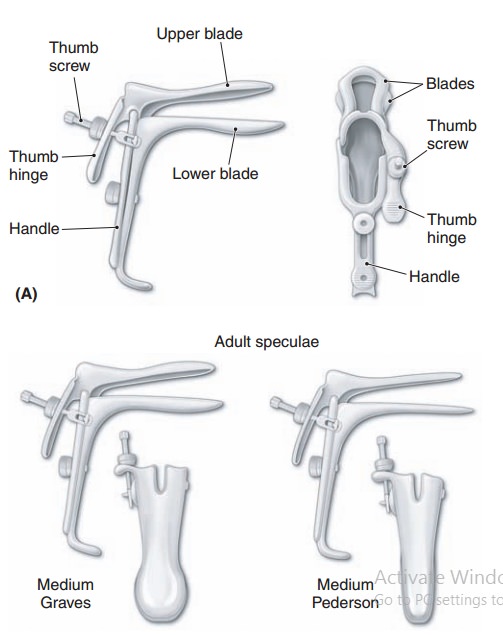
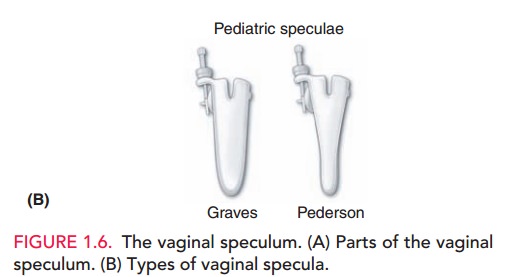
The Graves speculum has blades that are wider, higher, and curved on the sides; it is more appropriate for most parous women. Its wider, curved blades keep the looser vaginal walls of multiparous women separated for visualization. A Pederson speculum with extra narrow blades may be used for visualizing the cervix in pubertal girls.
The speculum should be warmed either with warm water or by holding it in the examiner’s hand. Warming the speculum is done for the comfort of the patient and to aid with insertion.
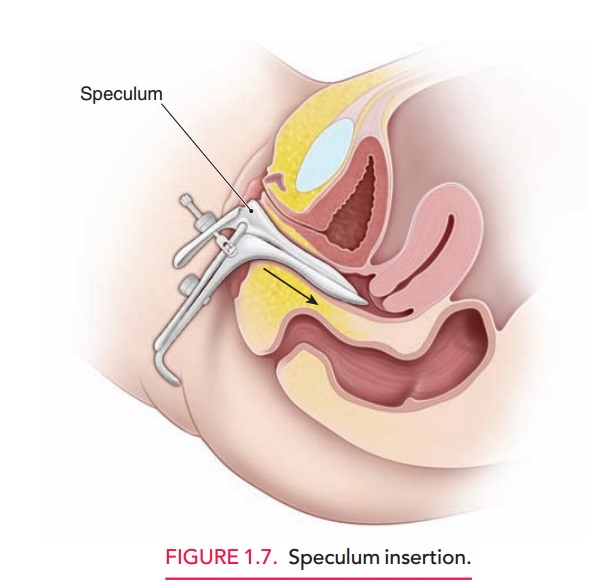
Insertion of the speculum should take into account thenormal anatomic relations, as illustrated in Figure 1.7. By in-serting the speculum along the axis of the vagina, minimal force is needed and comfort is maximized. Until recently, use of lubricants was avoided because of interference with cytologic interpretation, although this is less of a concern with liquid-based Pap test techniques. Situations that may require lubricant use are encountered infrequently and in-clude some prepubertal girls, some postmenopausal women, and patients with irritation or lesions of the vagina.
Most physicians find that control of pressure and movement of the speculum are facilitated by holding the speculum with the dominant hand. The speculum is held by the handle with the blades completely closed. The first two fingers of the opposite hand are placed on the perineum laterally and just below the introitus; pressure is applied downward and slightly inward until the introi-tus is opened slightly. If the patient is sufficiently re-laxed, this downward pressure on the perineum causes
The speculum is initially inserted in a hori-zontal plane with the width of the blades oblique to the verti-cal axis of the introitus. The speculum is then directed posteriorly at an approximately 45-degree angle from hori-zontal; the angle is adjusted as the speculum is inserted, so that the speculum slides into the vagina with minimal resistance. If the patient is not relaxed, posterior pressure from a finger inserted in the vagina sometimes relaxes the per-ineal musculature.
As the speculum is inserted, a slight continuous downward pressure is exerted so that distension of the perineum is used to create space into which the speculum may advance. Taking ad-vantage of the distensibility of the perineum and vagina posterior to the introitus is a crucial concept for the effi
Pressure superiorly causes pain in the sensitive area of the urethra and clitoris. The speculum is inserted as far as it will go, which in most women means insertion of the entire speculum length. The speculum is then opened in a smooth and deliberate fashion. With slight tilting of the speculum, the cervix slides into view between the blades of the speculum. The speculum is then locked into the open position using the thumbscrew. Failure tofind the cervix most commonly results from not having the speculum inserted far enough. Keeping the speculum fullyinserted while opening the speculum does not result in discomfort.
When the speculum is locked into position, it usually stays in place without being held. For most patients,
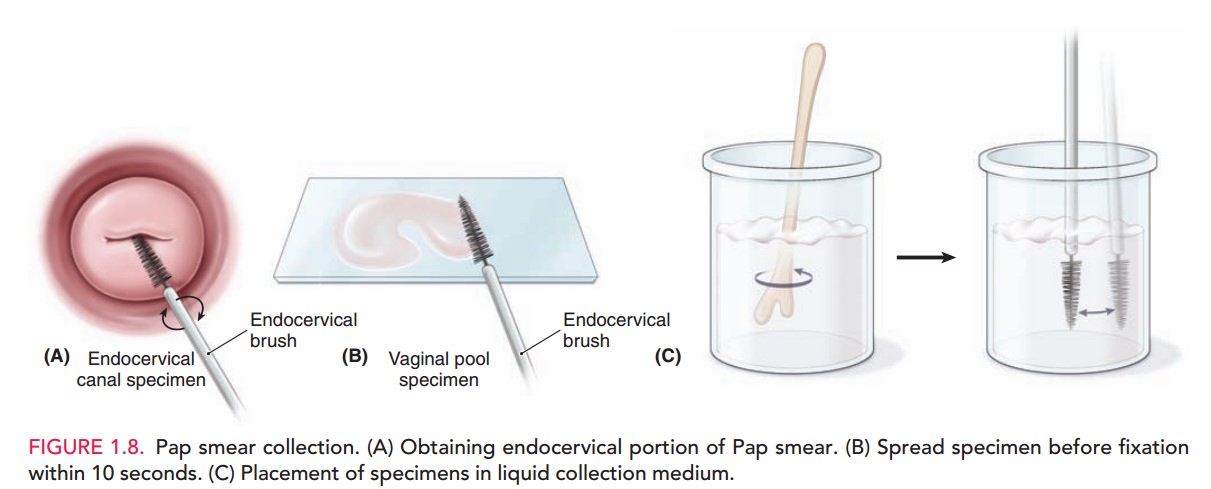
the speculum is opened sufficiently by use of the upper thumbscrew. In some cases, however, more space is re-quired. This may be obtained by gently expanding the ver-tical distance between the speculum blades by use of the screw on the handle of the speculum. With the speculum in place, the cervix and the deep lateral vaginal vault may be inspected and specimens obtained. Before obtaining tissue samples for the Pap test, the patient should be told that she may feel a slight “scraping” sensation, but no pain. Specimens are collected to fully evaluate the transforma-tion zone, where cervical intraepithelial neoplasia is more likely to be encountered. Specimens are obtained from the exo-cervix and endocervix and either plated on slides which are im-mediately fixed with a preservative spray or placed in a liquid collection medium (Fig. 1.8).
Speculum withdrawal also allows for inspection of the vaginal walls. After telling the patient that the speculumis to be removed, the blades of the speculum are opened slightly by putting pressure on the thumb hinge, and the thumbscrew is completely loosened. Opening the specu-lum blades slightly before starting to withdraw the specu-lum avoids pinching the cervix between the blades. The speculum is withdrawn approximately 1 inch before pres-sure on the thumb hinge is slowly released. The specu-lum is withdrawn slowly enough to allow inspection of the vaginal walls. The blades of the speculum are natu-rally brought together by vaginal wall pressure. As the endof the speculum blades approaches the introitus, there should be no pressure on the thumb hinge, otherwise the anterior blade can flip up, hitting the sensitive vaginal, urethral, and clitoral tissues.
Related Topics