Chapter: Nutrition and Diet Therapy: Diet During Childhood and Adolescence
Special Considerations for the Adolescent Related to Nutrition Concerns
SPECIAL CONSIDERATIONS
FOR THE ADOLESCENT RELATED TO NUTRITION CONCERNS
Adolescence is a
stressful time for most young people. They are unexpectedly faced with numerous
physical changes, an innate need for independence, increased work and
extracurricular demands at school, in many cases jobs, and social and sexual
pressures from their peers. For many teens, such stress can cause one or more
of the following problems.
Anorexia Nervosa
In general, adolescent
boys in the United States are considered well nourished. Studies show, however,
that girls sometimes have diets deficient in calories and protein, iron,
calcium, vitamin A, or some of the B vitamins.
These deficiencies can
be due to poor eating habits caused by concern about weight. A moderate concern
about weight is understandable and possibly even beneficial, provided it does
not cause diets to be deficient in essential nutri-ents or lead to a
potentially fatal condition called anorexia nervosa.
Anorexia nervosa,
commonly called anorexia, is a
psychological disorder more common to women than men. It can begin as early as
late childhood, but usually begins during the teen years or the early twenties.
It causes the client to drastically reduce calories, causing altered
metabolism, which results in hair loss, low blood pressure, weakness, amenorrhea, brain damage, and
even death.
The causes of anorexia
are unclear. Someone with this disorder (an anorexic) has an inordinate fear of
being fat. Some anorexics have been over-weight and have irrational fears of
regaining lost weight. Some young women with demanding parents perceive this as
their only means of control. Some may want to resemble slim fashion models and
have a distorted body image, where they see themselves as fat even though they
are extremely thin. Some fear growing up. Many are perfectionistic
overachievers who want to control their body. It pleases them to deny themselves
food when they are hungry.
These young women
usually set a maximum weight for themselves and become an expert at “counting
calories” to maintain their chosen weight. They also often exercise excessively
to control or reduce their weight. If the weight declines too far, the anorexic
will ultimately die.
Treatment requires the
following:
· Development of a
strong and trusting relationship between the client and the health care
professionals involved in the case.
· That the client learn
and accept that weight gain and a change in body contours are normal during
adolescence.
· Nutritional therapy so
the client will understand the need for both nutrients and calories and how
best to obtain them.
· Individual and family
counseling so the problem is understood by everyone.
· Close supervision by
the health care professional.
· Time and patience from
all involved.
Bulimia
Bulimia
is a syndrome in which the client alternately binges and purges by inducing
vomiting and using laxatives and diuretics to get rid of ingested food.
Bulimics are said to fear that they cannot stop eating. They tend to be high
achievers who are perfectionistic, obsessive, and depressed. They generally
lack a strong sense of self and have a need to seem special. They know their
binge–purge syndrome is abnormal but also fear being overweight. This condition
is more common among women than men and can begin any time from the late teens
into the thirties.
A
bulimic usually binges on high-calorie foods such as cookies, ice cream,
pastries, and other “forbidden” foods. The binge can take only a few moments or
can run several hours—until there is no space for more food. It occurs when the
person is alone. Bulimia can follow a period of excessive dieting, and stress
usually increases the frequency of binges.
Bulimia
is not usually life-threatening, but it can irritate the esophagus and cause
electrolyte imbalances, malnutrition, dehydration, and dental caries.
Treatment
usually includes limiting eating to mealtimes, portion control, and close
supervision after meals to prevent self-induced vomiting. Diet therapy helps
teach the client basic nutritional facts so that he or she will be more
inclined to treat the body with respect. Psychological counseling will help the
client to understand his or her fears about food. Group therapy also can be
helpful.
Both
bulimia and anorexia can be problems that will have to be confronted throughout
the client’s life.
Overweight
Being overweight
during adolescence is particularly unfortunate because it is apt to diminish
the individual’s self-esteem and, consequently,
can exclude her or him from the normal social life of the teen years, further
diminishing self-esteem. Also, it tends to make the individual prone to
overweight as an adult.
Although numerous
studies have been done, the cause of being over-weight is difficult to
determine. Heredity is believed to play a role. Just as one inherits height,
color of hair, or artistic talents, it appears that one may inherit the
tendency (or lack of it) to be overweight. Overfeeding during infancy and
childhood also can be a contributing factor. Then, once a person is overweight,
the overweight itself contributes further to the problem.
For example, if a
teenager becomes the center of his classmates’ jokes, he or she may prefer to
spend time alone, perhaps watching television and finding comfort in food. This
behavior adds more calories, reduces activity, and, thus, worsens the
condition.
The problem of being
overweight during adolescence is especially diffi-cult to solve until the
individual involved makes the independent decision tochange lifestyle habits.
After making such a decision, the teenager should see a physician to ensure
that his or her health is good. The health care provider can play an important
role by offering guidance on changing eating habits, increasing exercise, and
adopting a healthier lifestyle.
Fast Foods
Many Americans have
become extremely fond of fast foods. Many others are
highly critical of their nutrient content. Examples of these foods—most of which
are favorites of teenagers—include hamburgers, cheeseburgers, French fries,
milkshakes, pizza, sodas, tacos, chili, fried chicken, and onion rings. Many
fast-food companies have the nutrient content of their products available to
help the public make better choices.
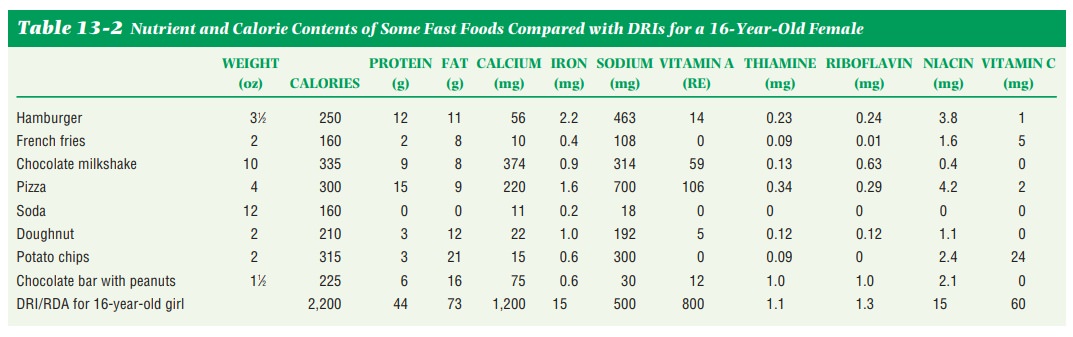
Generally speaking,
fast foods are excessively high in fat and sodium, as well as calories, and
contain only limited amounts of vitamins and minerals (other than sodium) and
little fiber. In Table 13-2, the nutrient content of some varieties of fast
foods are shown compared with the DRIs for a 16-year-old girl. This shows the
potential for problems with a diet that regularly consists of these foods to
the exclusion of others.
Nevertheless, these
foods are more nutritious than sodas, cakes, and candy. When used with
discretion in a balanced diet, they are not harmful. However, teens often use
fast foods as a snack to hold them over until dinner, and this results in
consumption of many extra calories.
Alcohol
In a process called fermentation, sugars and starches
can be changed to alcohol. Enzyme action causes this change. Alcohol is
typically made from fruit, corn, rye, barley, rice, or potatoes. It provides 7
calories per gram but almost no nutrients.
Alcohol is a substance
that can have serious side effects. Initially, it causes the drinker to feel
“happy” because it lowers inhibitions. This feeling affects the drinker’s
judgment and can lead to accidents and crime. Ultimately, alcohol is a
depressant; continued drinking leads to sleepiness, loss of consciousness, and,
when too much is consumed in a short period, death.
Abuse (overuse) of
alcohol is called alcoholism. Alcoholism can
destroy the lives of families and devastate the drinker’s nutritional status
and thus health. It affects absorption and normal metabolism of glucose, fats,
proteins, and vitamins. When thiamine and niacin cannot be absorbed, the cells
cannot use glucose for energy. Blood cells, which depend on glucose for energy,
are particularly affected. Over time, if alcohol abuse continues, fat will
accu-mulate in the liver, leading to cirrhosis. Alcohol causes
kidneys to excrete larger-than-normal amounts of water, resulting in an
increased loss of minerals. In a poor nutritional state, the body is less able
to fight off disease.
In addition,
excessive, long-term drinking can cause high blood pressure and can damage the
heart muscle. It is associated with cancer of the throat and the esophagus and
can damage the reproductive system.
The risks to the
drinker are obvious. When a pregnant or lactating woman drinks, however, she
puts the fetus or the nursing infant at risk as well. Alcohol can lower birth
weight and cause fetal alcohol syndrome or fetal alcohol effect, with related
developmental disorders.
Unfortunately, many
teenagers ignore the dangers of alcohol and use it in an effort to appear
adult. In addition to the damage to their own health and the accidents and the
random acts of violence caused by their drinking, their behavior inspires younger
children to emulate them. The health professional is in a good position to
spread the message that alcohol is a substance and can cause severe economic
and family problems, as well as addiction, disease, and death.
Marijuana
Marijuana use
continues to increase among teenagers. Marijuana increases appetite, especially
for sweets. One marijuana cigarette is as harmful as four or five tobacco
cigarettes because the marijuana smoke is held in the lungs for a longer period
of time. As marijuana is smoked, the lungs absorb the fat-soluble active
ingredient, delta-9-tetrahydrocannabinol (THC), and store it in the fat
(Indiana Prevention Resource Center, 2003). Experts believe that the use of
marijuana can lead to the use of other drugs such as cocaine. Common street
names for marijuana include grass, weed, pot, and dope.
Cocaine
Cocaine is highly
addictive and extremely harmful. It causes restlessness, heightened
self-confidence, euphoria, irritability, insomnia, depression, confu-sion,
hallucinations, loss of appetite, and a tendency to withdraw from normal
activities. Cocaine can cause cardiac irregularities, heart attacks, and
cardiac arrests resulting in death. Weight loss is very common, mostly because
it decreases appetite; addicts would give up food for the drug. The smokable
form of cocaine is crack, which is
more addictive than any other drug. It is estimated that half of all crimes
against property committed in major cities are related to the use of crack
cocaine and the addict’s need for money to buy the drug.
Tobacco
Cigarette smoking is
addictive. Cigarette smoking by teenagers is very preva-lent. Teenagers smoke
to “be cool,” to look older, because they think it will help them lose weight,
or because of peer pressure. Smoking can influence appetite, nutrition status,
and weight. Smokers need the DRI for vitamin C plus 35 mg because smoking
alters the metabolism. Low intakes of vitamin C, vitamin A, beta-carotene,
folate, and fiber are common in smokers. Smoking increases the risk of lung
cancer and heart disease.
Other Addictive Drugs
Methamphetamine is the
most potent form of amphetamines. Amphetamines cause heart, breathing, and
blood pressure rates to increase. The mouth is usually dry, and swallowing is
difficult. Urination is also difficult. Appetite is depressed. The users’
pupils are dilated, and reflexes speed up. As the drug wears off, feelings of
fatigue or depression are experienced. Street names include crank, speed,
crystal, meth, zip, and ice.
Inhalants are
chemicals whose fumes are inhaled into the body and produce mind-altering
effects. Some inhalants are gasoline, lighter fluid, tool-cleaning solvents,
model airplane glue, typewriter correction fluid, and permanent ink in felt-tip
pens. Inhalants are both physically and psychologically addictive. Indi-viduals
who inhale may risk depression and apathy, nosebleeds, headaches, eye pain,
chronic fatigue, heart failure, loss of muscle control, and death.
Nutrition for the Athlete
Good nutrition during
the period of life when one is involved in athletics can prevent unnecessary
wear and tear on the body as well as maintain the athlete in top physical form.
The specific nutritional needs of the athlete are not numerous, but they are
important. The athlete needs additional water, calories, thiamine, riboflavin,
niacin, sodium, potassium, iron, and protein.
The body uses water to
rid itself of excess heat through perspiration. This lost water must be
regularly replaced during the activity to prevent dehydra-tion. Plain water is
the recommended liquid because it rehydrates the body more quickly than
sweetened liquids or the drinks that contain electrolytes. The “electrolyte”
drinks are useful to replenish fluids after an athletic event but not during
one. Salt tablets are not recommended because despite the loss of salt and
potassium through perspiration, the loss is not equal to the amount contained
in the tablets. If there is an insufficient water intake, these salt tablets
can increase the risk of dehydration.
The increase in
calories depends on the activity and the length of time it is performed. The
requirement could be double the normal, up to 6,000 calories per day. Because
carbohydrates, not protein, are used for energy, the normal diet proportions of
50% to 55% carbohydrate, 30% fat, and 10% to 15% protein are advised.
There is an increased
need for B vitamins because they are necessary for energy metabolism. They are
provided in the breads, cereals, fruits, and vegeta-bles needed to bring the
calorie count to the total required. Some extra protein is used during
training, when muscle mass and blood volume are increasing. This amount is
included in the DRI for age and is provided in the normal diet. Protein needs
are not increased by physical activity. In fact, excess protein can cause
increased urine production, which can lead to dehydration.
The minerals sodium
and potassium are needed in larger amounts because of loss through
perspiration. This amount of sodium can usually be replaced just by salting
food to taste, and orange juice or bananas can provide the extra potassium.
A sufficient supply of
iron is important to the athlete, particularly to the female athlete. Iron-rich
foods eaten with vitamin C–rich foods should provide sufficient iron. The onset
of menstruation can be delayed by the heavy physical activity of the young
female athlete, and amenorrhea may occur in those already menstruating.
When weight is a
concern of the athlete, such as with wrestlers, care should be taken that the
individual does not become dehydrated by refusing liquids in an effort to “make
weight” for the class.
When weight must be
added, the athlete will need an additional 2,500 calories to develop 1 pound of
muscle mass. The additional foods eaten to reachthis amount of calories should
contain the normal proportion of nutrients. A high-fat diet should be avoided
because it increases the potential for heart disease. Athletes should reduce
calories when training ends.
In general, the
athlete should select foods using MyPyramid. The pregame meal should be eaten 3
hours before the event and should consist primarily of carbohydrates and small
amounts of protein and fat. Concentrated sugar foods are not advisable because
they may cause extra water to collect in the intestines, creating gas and
possibly diarrhea.
Glycogen loading (carboloading) is sometimes used for
long activities.To increase muscle stores of glycogen, the athlete begins 6
days before the events. For 3 days, the athlete eats a diet consisting of only
10% carbohydrate and mostly protein and fat as she or he performs heavy
exercise. This depletes the current store of glycogen. The next 3 days, the
diet is 70% carbohydrate, and the exercise is very light so that the muscles
become loaded with glycogen. This practice may cause an abnormal heartbeat and
some weight gain.
Currently, it is
recommended that the athlete exercise heavily and eat carbohydrates as desired.
Then, during the week before the competition, exer-cise should be reduced. On
the day before competition, the athlete should eat a high-carbohydrate diet and
rest.
After the event, the
athlete may prefer to drink fruit juices until relaxed and then satisfy the
appetite with sandwiches or a full meal. Many athletes will use “power drinks”
or “energy drinks,” which are not any better than soda and contain mostly sugar
and empty calories.
There are no magic
potions or diet supplements that will increase an athlete’s prowess, as may be
touted by health food faddists. Steroid
drugs should not be used to build muscles (Figure 13-6). They can affect the
fat content of the blood, damage the liver, change the reproductive system, and
even alter facial appearance. Good diet, good health habits, and practice
combined with innate talent remain the essentials for athletic success.

Related Topics