Chapter: Obstetrics and Gynecology: Endometriosis
Signs and Symptoms of Endometriosis
SIGNS AND SYMPTOMS
Women
with endometriosis demonstrate a wide variety of symp-toms. The
nature and severity of symptoms may not matcheither the location or extent of the
disease. Women with grossly extensive endometriosis may have few symptoms,
whereas those with minimal gross endometriosis may have severe pain. Endometriosis may also be asymptomatic.
The pain associated with endometriosis is thought to depend more upon the depth
of invasion of the implants rather than on the number or extent of the
superficial implants. The classicsymptoms
of endometriosis include progressive dysmenorrhea
and deep dyspareunia.Some
patients experience chronic,unremitting pelvic discomfort along with
dysmenorrhea and dyspareunia. Chronic pelvic pain may be related to the
adhesions and pelvic scarring found in association with endometriosis.
Dysmenorrhea caused by
endometriosis is not directly related to the amount of visible disease. In many
women with endometriosis, the dysmenorrhea worsens over time. Endometriosis
should be considered a possible etiology in patients who present with
dysmenorrhea that does not respond to oral contraceptives or nonsteroidal
anti-inflammatory agents (NSAIDs). Dyspareunia is often associated with
uterosacral or deep posterior cul-de-sac involvement with endometriosis. The
dyspareunia is typically reported on deep penetration, although there is no
correlation between dyspareunia and the extent of endometriosis.
Infertility is more frequent in women with endometriosis, although a cause-and-effect relationship has not been established. With extensive disease, pelvic scarring and adhesions that distort pelvic anatomy may cause infertility, but the cause of infertility in women with minimal endometriosis is unclear. Prostaglandins and autoantibodies have been implicated, but these relationships remain unproven.
In some cases, infertility may be
the only complaint, and endometriosis is discovered at the time of laparoscopic
evaluation as part of the infertility workup. The presence of endometriosis in
asymptomatic infertility patients varies between 30% and 50%. Other,
less-common symptoms of endometriosis in-clude gastrointestinal symptoms, such
as rectal bleeding and dyschezia
(painful bowel movements) in patients with endometrial implants on the bowel
and urinary symptoms such as hematuria in patients with endometrial implants on
the bladder or ureters. Occasionally, patients may present with an acute
abdominal emergency, which may be associ-ated with the rupture or torsion of an
endometrioma.
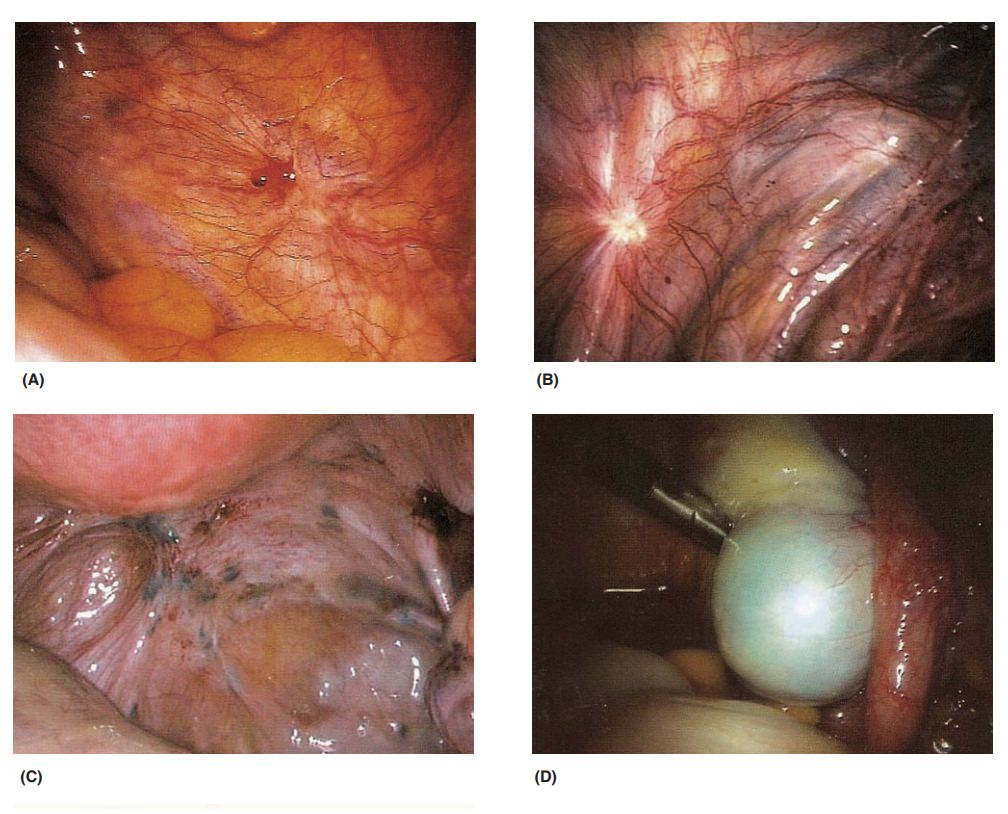
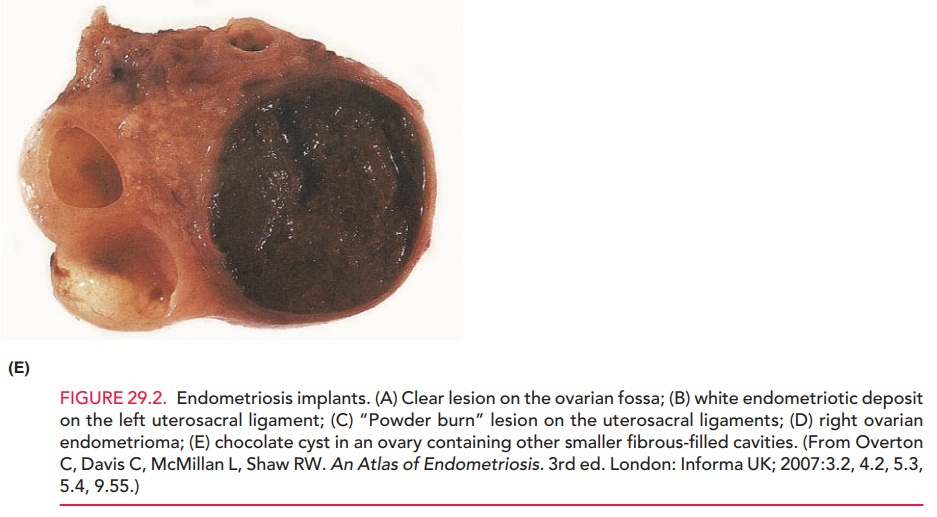
Pelvic examination may reveal the
“classic” sign of uterosacral nodularity associated with endometriosis, but it
is often absent even when substantial gross endometriosis is discovered at
surgery. The uterus may be relatively fixed and retroflexed in the pelvis
because of extensive adhesions. Ovarian endometriomas may be tender, palpable,
and freely mobile in the pelvis, or adhered to the posterior leaf of the broad
ligament, the lateral pelvic wall, or in the posterior cul-de-sac (see Fig.
29.2).
Related Topics